
Submitted by Dawn on Wed, 05/23/2012 - 20:57
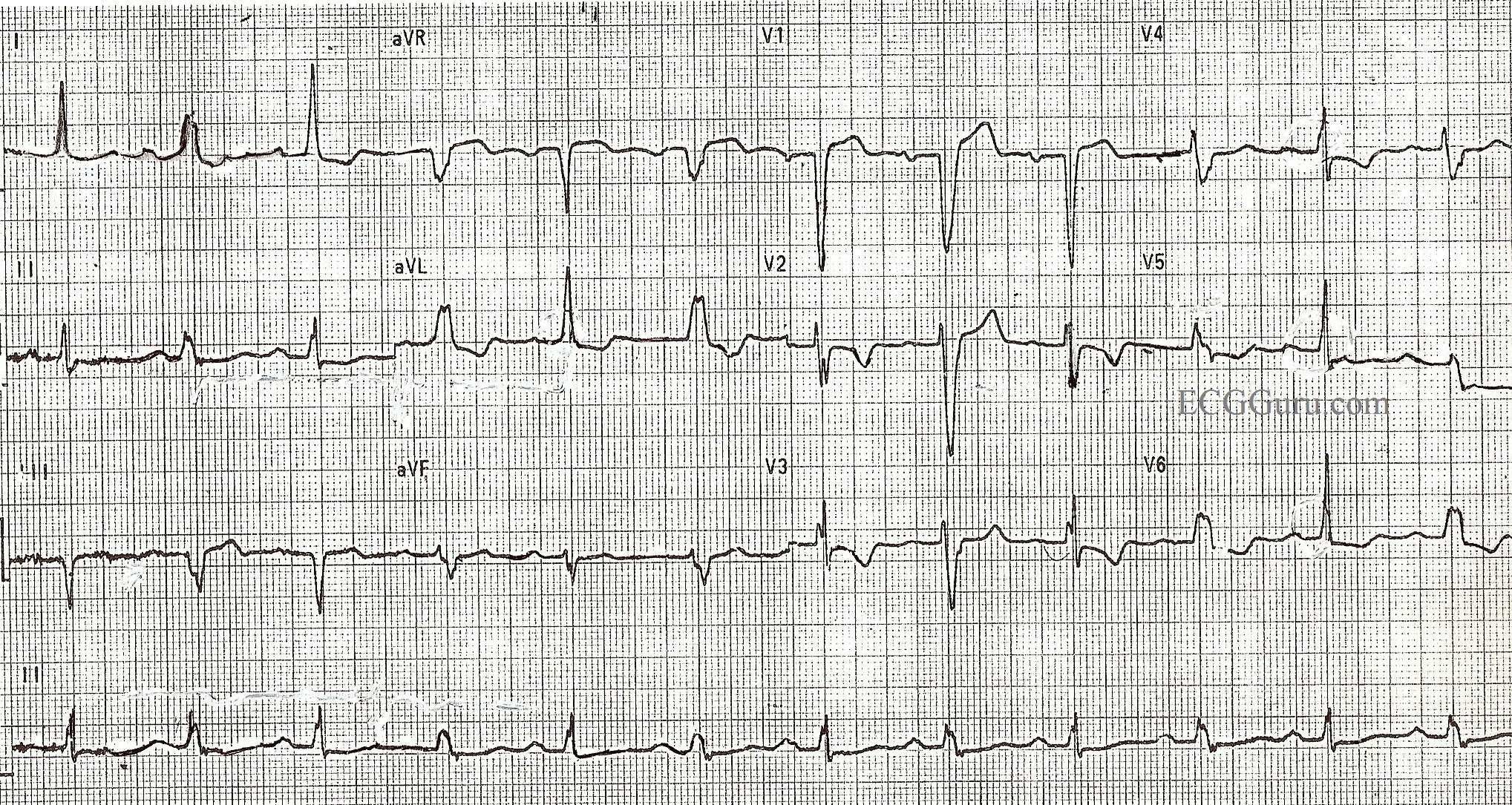
This patient suffered a recent anterior-septal wall M.I., which can be seen as slight ST elevation in V1 and ischemic T wave inversions in V2 through V4. The patient has developed an intermittent left bundle branch block as a result of this M.I. Every other beat is conducted in a left bundle branch block pattern, as the LBB cannot repolarize in time for each beat. The criteria for LBBB are: wide QRS, supraventricular rhythm, and negatively-deflected QRS in V1 with a positive QRS in V6 and Lead I.
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Alternating BBB aberrancy / concealed transseptal conduction
In his textbook "Electrocardiography of Clinical Arrhythmias", Dr. Charles Fisch considers this pattern to be a subcategory of "electrical alternans" even though that term is usually reserved for use with either pericardial effusion and orthodromic tachycardia. Dr. Fisch's suggested cause for the alternating LBBB aberrancy is a mechanism known as "concealed transseptal conduction". Just over two months ago I contributed a 12-lead ECG to The Guru of a patient having an acute inferior infarction complicated by LBBB. Some time prior to the infarction, the patient exhibited an identical pattern of alternating LBBB aberrancy as seen in the ECG above. Subsequently, the patient's LBBB was permanent (i.e., fixed) following the infarction. Such infarctions often wreak havoc on the bundle-branches.
http://www.ekgguru.com/content/left-bundle-branch-block-acute-inferior-wall-mi
Jason E. Roediger - Certified Cardiographic Technician (CCT)
[email protected]