
Submitted by Dr A Röschl on Tue, 01/14/2025 - 01:53
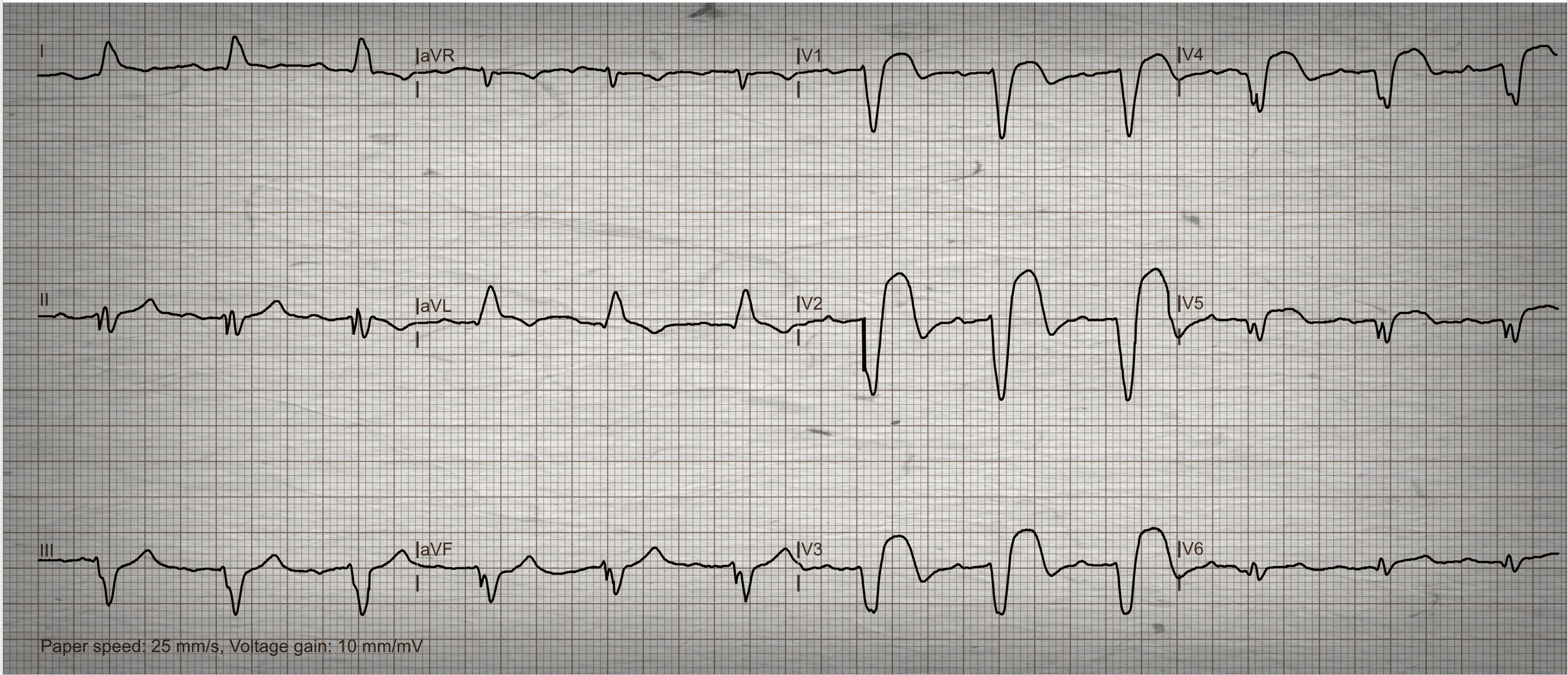
This ECG was sent to me by a friend, I don't know if he did it himself. The question was whether a heart attack can be recognized here. The patient is a 55-year-old man who has typical angina pectoris lasting more than 1 hour.
What can you answer?
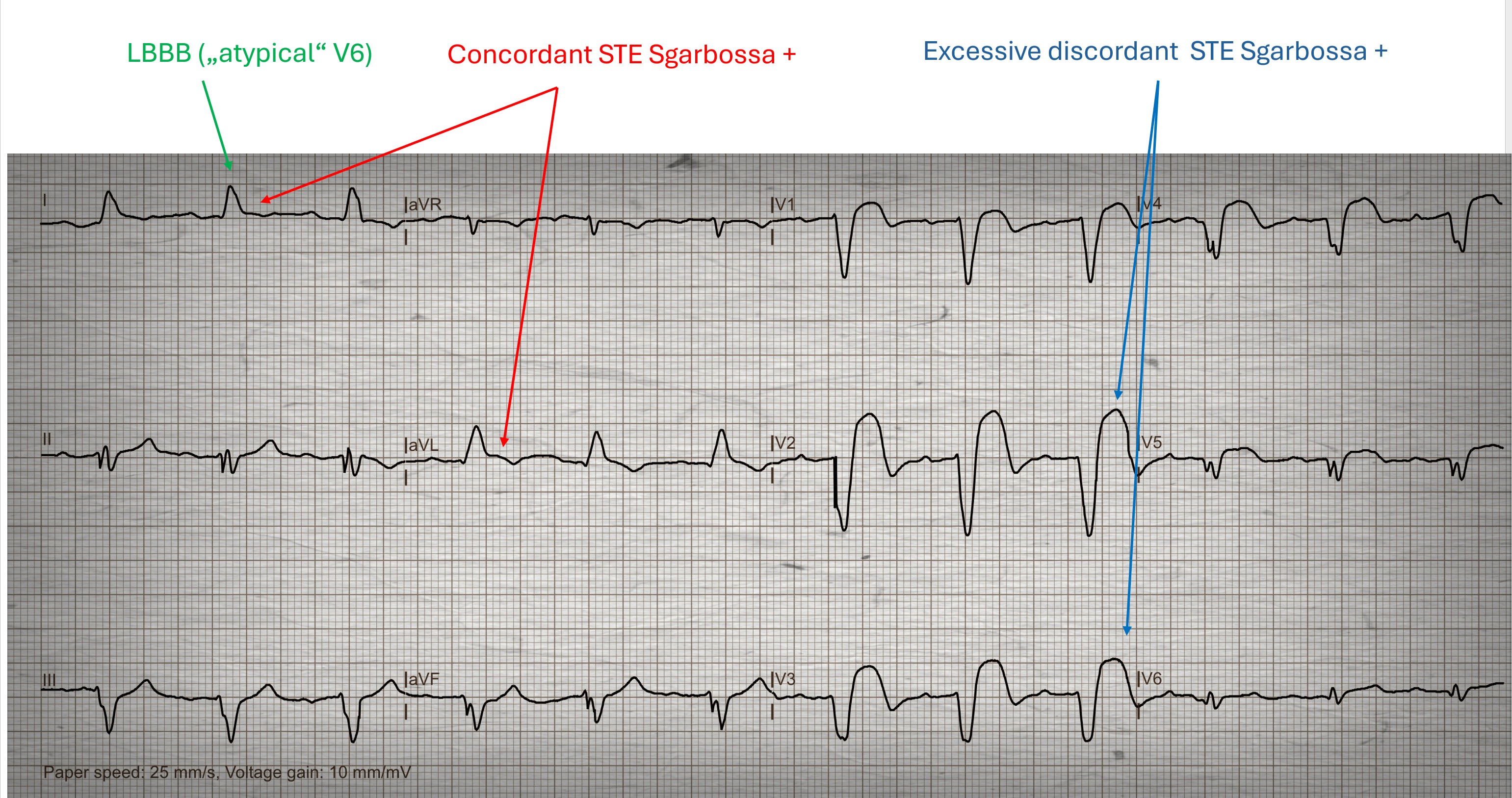
We can see a SR with a slightly prolonged PR interval (1st degree AVB). The limb leads show a typical left bundle branch block. This cannot be seen in the precordial leads (V6!). In an LBBB, the ST segments in I and aVL should point in the opposite direction to the QRS complexes, here the ST segments are slightly concordant. In the precordial leads, excessively discordant ST segment elevations in V2-V4 are noticeable. Several Sgarbossa criteria are therefore positive here, which allows us to assume an acute AWMI.
The original Sgarbossa Criteria were established in 1996 by Elena B Sgarbossa and her colleagues. The criteria are meant to help diagnose acute M.I. in the presence of left bundle branch block. https://pmc.ncbi.nlm.nih.gov/articles/PMC5056892/ In 2012, Dr. Stephen Smith and colleagues publishedhtt the Smith-modified Sgarbossa Criteria, which improves accuracy. Smith et al had the advantage of following patients from the ED through cath lab results. https://litfl.com/sgarbossa-criteria-ecg-library/
Rate this content:
-

- Dr A Röschl's blog
- Log in or register to post comments
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.