
Submitted by Dawn on Tue, 02/03/2015 - 19:06




This series of strips was donated by Arnel Carmona, and was taken from a patient admitted to the hospital for a urinary tract infection. No other history is known. On close examination of this rhythm what do we see?
Strip 1: Narrow-complex tachycardia with NO apparent P waves.
Strip 2: Some irregularity, with long regular groups and still NO P waves.
Strips 3 & 4: Grouped beating.
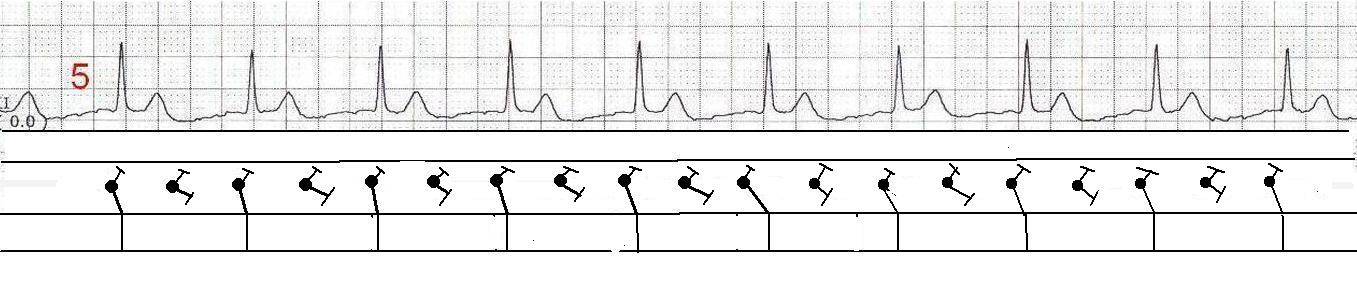
Strip 5: A narrow-complex rhythm that is approximately ½ the rate of Strip 1.
When grouped beating is seen, one should always suspect Wenckebach conduction. Wenckebach conduction (progressively longer conduction times through the A-V conduction system) can occur in rhythyms other than sinus rhythm. Without P waves and PR intervals, GROUPED BEATING is our major clue to Wenckebach conduction.
This patient has an underlying atrial fibrillation – hence no P waves. Fine fibrillatory waves can be seen, but artifact can cause the same appearance. So, why is there no irregular irregularity? There is another rhythm at work here along with the atrial fibrillation. Junctional tachycardia is seen in Strip 1. When two tachycardias coexist, one from above the AV junction, and one from below, the rhythm can be called a “double tachycardia”. This particular combination often happens in patients with digitalis toxicity.
In some cases, a complete heart block at the level of the atrial conduction fibers or the AV node causes two rhythms to operate independently. Any supraventricular rhythm, including atrial fib, can occur with a complete heart block, in which case we would see an “escape” rhythm. Escape rhythms are usually slow, either idiojunctional (40-60 bpm) or idioventricular (< 40 bpm).
Let’s look at each of the strips in detail. We will begin with the hypothesis that this is atrial fibrillation with concurrent junctional tachycardia at around 150 bpm. I will include laddergrams to illustrate my view of what is happening.
Strip 1 : Junctional tachycardia at around 148-150/min. Differential diagnosis would include sinus tach with 1st degree AV block, but we have no evidence in this strip of P waves in the T waves. There is presumably an entrance block to the AV node, preventing retrograde P waves from the AV junction from entering the atria.
Strip 2: In this strip, I feel less confident of my hypothesis, but have been able to construct a laddergram that is consistent with a fib and junctional tach with Wenckebach exit block. I would, as always, welcome input.
Strip 3: Now, the grouped beating is very evident. I have mapped out on the laddergram where the beats originate in the AV junction, and where they become a QRS. You can see progressive prolongation in these impulses traveling to the ventricles. There are no P waves because of the atrial fib and the block preventing junctional beats from traveling backward into the atria.
Strip 4: The group beating has taken the form of couplets. The rhythm looks like sinus with PACs, but WAIT …… no P waves, remember?
Strip 5: Now, the junctional beats are conducting 2:1, and the rate is half what it was in Strip 1, when conduction was 1:1.
These links may be helpful to you. Discussion of double tachycardia with a fib and junctional tach in EP Europace. Discussion of atrial fib and Wenckebach in digitalis toxicity by Dr. Ken Grauer. Original posting of strips on Arnel Carmona's website, ECG Rhythms. These strips are the property of Arnel Carmona and should be used only in an educational context. For any other use, contact [email protected].
Thanks so much to Arnel Carmona for this excellent teaching series. We hope you will add your comments and/or questions below.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Excellent Case!
Dawn...
Thanks for such a thought-provoking (and brain-teasing) case.
I certainly agree with your interpretations and diagrams in strips 1, 3-5.
First, there is definitely a complete block between atria and ventricles; otherwise, the fibrillatory waves would keep resetting the junctional pacemaker (assuming no entrance block).
I think I may have an explanation for your findings in strip #2.
Whenever you have a second degree block with greater than a 4:1 conduction you are usually looking at a multi-level AV (or AV-junctional) block. Regarding strip #2 (and I think you have diagrammed it well in a single-level fashion), if we postulate a dual level AV/junctional block with a Wenckebach conduction having a longer episode in the the upper tier and a Wenckebach conduction with a shorter episode in the lower tier, you will get exactly the pattern displayed in the first section of the tracing #2. The Wenckebach in the lower tier - having a shorter episode - will end sooner, accounting for the pause after the sixth QRS. The Wenckebach episode in the upper tier, however, is not finished yet and has one more conducted H' before ending its sequence. Hence, the next pause followed by a junctional beat with the shortest H'-R interval, which starts both Wenckebach sequences once more. Both tiers share the same complexes until their endings. It is how they end that makes the difference. If the Wenckebach with the shorter episode were in the upper tier, you would have no way of knowing what was in the lower tier because the upper tier, by ending, resets the AV/junction for a new Wenckebach episode (when both tiers manifest Wenckebach conduction).
The H'-R interval of complex #8 is longer than the previous H'-R interval. If this were a simple 2:1 block or even the beginning of another Wenckebach sequence, the H'-R interval should be shorter. The only reason for this particular H'-R interval to be longer would be if it were ending a Wenckebach sequence.
Thanks to all for a very enlightening and challenging website!
Jerry. W. Jones, MD
Jerry W. Jones MD FACEP FAAEM
https://www.medicusofhouston.com
Twitter: @jwjmd
Addendum to my comment
You can also view this as a three-level AV/junctional block with the third degree block of the atrial impulses in the first tier and the two Wenckebach episodes in the second and third tiers. There are some researchers/electrophysiologists that feel there are always three levels of conduction, though the actual delays or blocks may occur in only one tier or in two adjacent tiers (1 and 2 or 2and 3) at a time.
Jerry W. Jones MD FACEP FAAEM
https://www.medicusofhouston.com
Twitter: @jwjmd
Thank you SO MUCH, Dr. Jones!
As I struggled to diagram the mechanism at work in Strip No. 2, I was not satisfied. It did not make "sense" to me that Beat #8 would have such a long H'-R interval, when it appeared to be the FIRST in a series! You have answered my questions beautifully. I do not have an EP background (only in recovering patients after procedures). I have done a bit of reading, but it is difficult without practice with a mentor. I am going to sit down and draw laddergrams with the AVJ tier divided - will that suffice for understanding the dual-tier blocks?
I try to include content on the ECG Guru for the very basic beginner and for more advanced practitioners. My MAIN goal is to provide good-quality teaching matrials that can be projected or reprinted so that teachers will have the materials they need. It is a bit distressing to me when I can't provide the "complete" answer, but this series was too good not to publish. Thank you so much for filling in that missing piece!
PS - We are always interested in having experts contribute to our "Ask the Expert" page. If you would be interested, please email me at [email protected]. Thanks again!!!
Dawn Altman, Admin
Thank You Dr. Jones! - re Multi-Level AV Block
I will echo Dawn's THANK YOU to you Dr. Jones for your wonderful explanation for rhythm strip #2. For most interpreters - I think simple recognition that a Wenckebach phenomenon is present is plenty, with consideration of likely multi-level involvement when periodicity is not quite typical. But it is great to have your specific description add light on this 2nd tracing.
Ken Grauer, MD www.kg-ekgpress.com [email protected]
Thanks to both of you for the kind words!
Dawn...
I think you have an excellent website that is so very challenging. You are doing an exemplary job and I congratulate you. I teach advanced electrocardiography and advanced dysrhythmia analysis here in Houston, Texas. There are only three websites that I recommend to my clients to continue their education at home: ECG Guru, Ken Grauer's website and Steven Smith's blog. All three adhere to very high standards. This is unfortunately too infrequent on the internet. There is a lot of misinformation about electrocardiography floating around out there.
I check in to your website fairly regularly but it's usually after everyone else has commented and all issues have usually been settled. Still, I find the site very informative and I hope to participate again soon.
Jerry W. Jones MD FACEP FAAEM
Jerry W. Jones MD FACEP FAAEM
https://www.medicusofhouston.com
Twitter: @jwjmd
1976 Kosowsky Article
The 1976 Kosowsky article that Dr. Grauer mentions is excellent! I have read it so many times over the years that I think it is burned into my retinas like a computer screen without a screensaver. I would also recommend the book "Electrocardiography of Arrhythmias" by Charles Fisch. I'm not sure if it is out of print or not. I got my copy from a medical library that was getting rid of some of their books. Now, don't confuse it with "Electrocardiography of CLINICAL Arrhythmias" by Fisch and Knoebel, which is really a "watered-down" version.
Jerry
Jerry W. Jones MD FACEP FAAEM
https://www.medicusofhouston.com
Twitter: @jwjmd
Thanks !
Thanks very much, Drs. Ken and Jerry, for the link to the article on multi-level blocks. I have read it, and now wish I could dig out all the old rhythm strips with a flutter and check them for Wenckebach periodicity! Being able to make a laddergram with more than one AV tier opens up a lot of possibilities. This reminds me that things we are taught before we are ready to learn them get pushed to the back corners of our minds. My teacher tried to explain this concept to me years ago, but I was not yet knowledgable enough to use it.
As as far as Dr. Fisch's text goes, it has been recommended to me many times. Alas, I have not found a used copy, and the new one is way outside the budget! :-). Will keep looking.
Thanks again!
Dawn Altman, Admin