
Submitted by Dawn on Tue, 10/07/2014 - 00:07
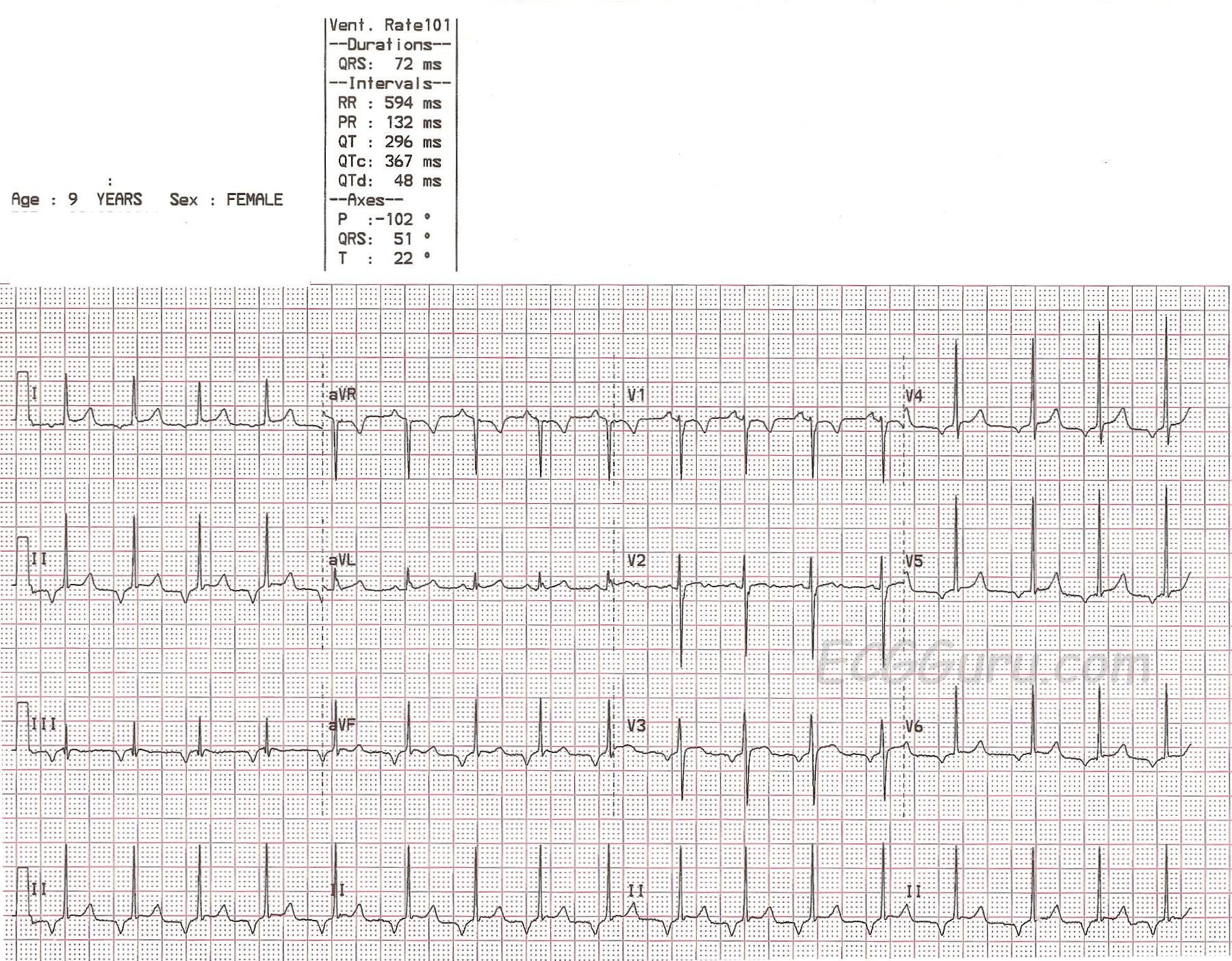
This ECG, taken from a nine-year-old girl, shows a regular rhythm with a narrow QRS and an unusual P wave axis. Unfortunately, we do not have any clinical information.
Normally, P waves are positive in Leads I, II, and aVF and negative in aVR. They can be biphasic in V1, but are usually positive in the rest of the precordial leads. . The P waves in this ECG are NEGATIVE in Leads I,II, III, aVF, and V3 through V6. This indicates RETROGRADE conduction through the atria - the impulse starts low and continues in a backward fashion through the atria. This tells us that the rhythm originated in the AV junction or low atria. The "junction" is usually defined as all of the complex AV node and the Bundle of His.
The literature over the years has been very confusing about the exact location of the "junctional" pacemakers. One commonly-accepted guideline was that a rhythm is "junctional" if there are retrograde P waves with a short PR interval, or a P wave that occurs within or after the QRS. A rhythm with a retrograde P wave and a NORMAL PR interval is said to be "low atrial", indicating that the ectopic pacemaker involved was located in the low atrium, producing retrograde conduction through the atria and normal delay through the AV node.
While both of these scenarios are plausible, it probably is not possible to say with certainty where the actual pacemaker is just by looking at the surface ECG. The AV node has been found to have pacemaking capability in all three of it's regions, and the Bundle of His is also able to produce ectopic impulses. PR intervals vary greatly, especially in pediatric patients, and can be influenced by heart size and heart rate. The retrograde conduction through the AV node toward the atria can occur over the fast or slow pathways. The "major" junctional pacemaker is thought to be in the proximal Bundle of His. Junctional or low atrial ectopic rhythms can occur because they override the rate of the sinus rhythm, following the rule that "The fastest pacemaker controls the heart". junctional rhythms can also occur as "escape" rhythms, only occurring because the sinus impulse has failed or been vlocked - often due to AV block.
Since the exact location of the ectopic pacemaker in this case cannot be determined without electrophysiology studies, it is important to evaluate the effect, if any, the rhythm is having on the patient. Since there is a P wave before every QRS, and the QRS complexes are narrow, it can be assumed that there will be no clinical effect on this patient. In addition, the rate is within normal range, and that is also unlikely to produce any clinical effect.
The causes of ectopic rhythms are many, and range from completely benign to serious. So, this child should be evaluated in light of her symptoms, history, and physical assessment.
The ECG remains a good teaching example of retrograde P waves that are NOT dissociated from the QRS complexes.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
A Slightly Fast and Variable AV Nodal Rhythm in a 9yo Child
As per Dawn - this tracing obtained from a 9-year old child shows what appears to be an AV Nodal rhythm - with 1:1 AV conduction from negative P waves preceding each of the inferior leads with a constant PR interval. I'd add the following points to Dawn's discussion.
Ken Grauer, MD www.kg-ekgpress.com [email protected]
Instructors' Collection ECG of the WEEK, October 7, 2014 __ Pedi
I'm not an expert.
It looks like a slightly variable supranodal or junctional paroxistic rythm or inferior posterior left atrial rythm. Maybe para and supranodal.
The variability may be to the respiration, it has 5 cicles repetion( in D II bellow ).
What about ST in D I, aVR and V 3 leads?
What about the variations in aVL and V 2?
Underlyng structural disease, intoxication?
Reply to drk
@ drk - I think we essentially agree about the rhythm - namely that it is difficult to be certain of etiology but that it may indeed by a slightly variable junctional rhythm in this 9-year old child (but that we can't rule out a low atrial source). There may be respiratory variation. I do see slight ST-T wave deviations. Some of this may reflect T of the abnormal P wave ... Overall - given that the patient is a 9-year old child, I don't think ST-T wave deviations are of clinical significance - but then again we unfortunately have no clinical correlation ...
Ken Grauer, MD www.kg-ekgpress.com [email protected]