
Submitted by Dawn on Sun, 06/08/2014 - 22:29
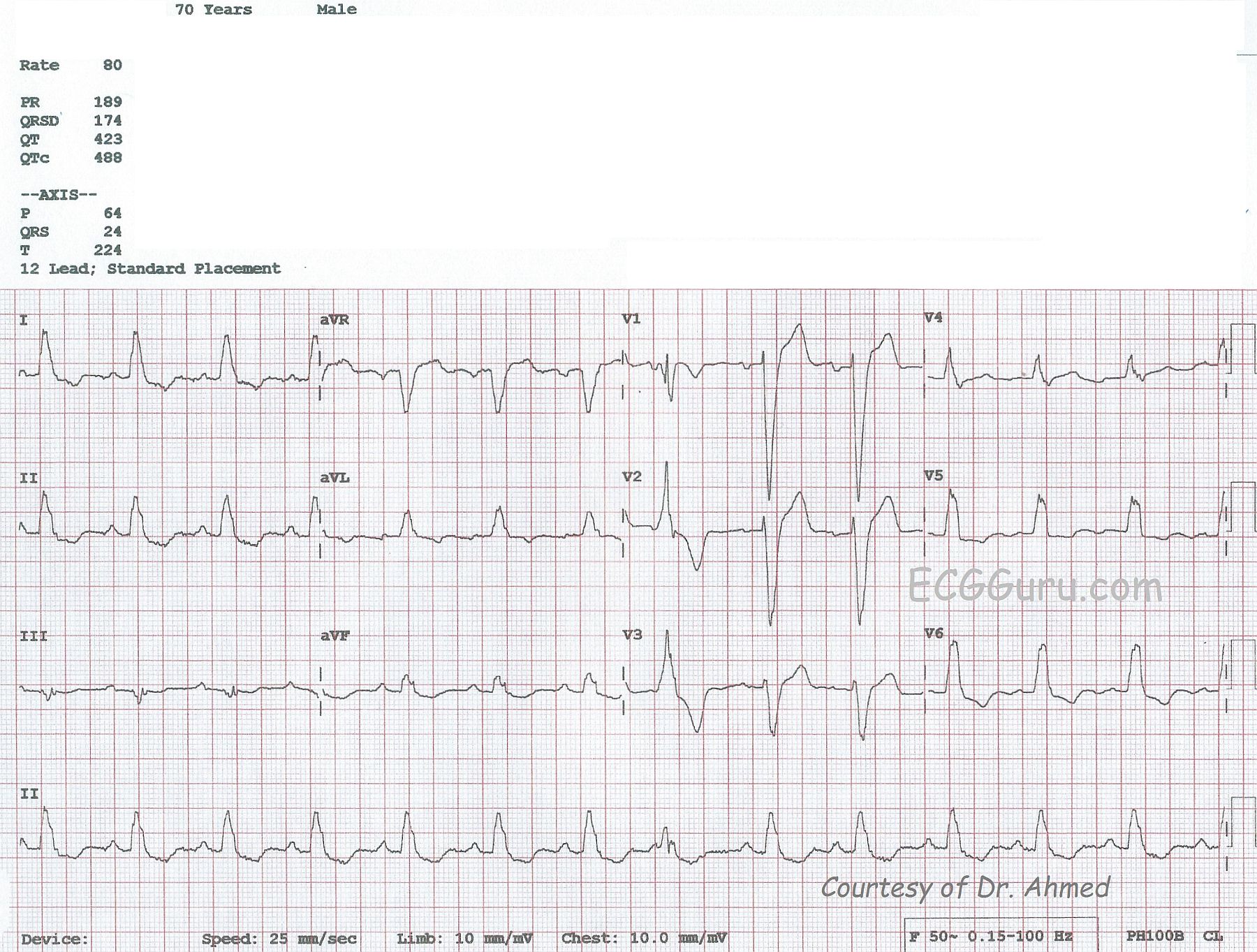
This ECG, kindly donated by Dr. Ahmed from India, is from a 70-year-old man shows a sinus rhythm at 80 bpm with left bundle branch block (LBBB), left atrial enlargement (LAE), and a premature ventricular contraction (PVC). The ECG criteria for LBBB is: 1) Wide QRS - greater than or equal to .12 seconds; 2) Supraventricular rhythm; 3) QRS that is negative in V1 and positive in Leads I and V6. In leads with a positive QRS, we will see some ST depression, and in leads with a negative QRS, some ST elevation. This is "normal" for the wide QRS rhythm, and does not indicate injury or ischemia, although it does not rule it out, either. LBBB is an indicator of cardiac disease, but not specific to one etiology.
There is a PVC seen as the 8th beat from the left, and it gives you a chance to show your students a wide-complex beat that is NOT associated with a P wave and is premature, compared to the wide-complex SINUS beats with LBBB. The PVC, being wide-complex, also has similar ST changes: the ST segments and T waves are DISCORDANT with the QRS complexes.
The P waves show some signs of enlargement of the left atrium. The P waves in Lead II are tall and pointed, and the P waves in V1 are biphasic. Left atrial enlargement in a patient with LBBB would not be surprising, as both are associated with left ventricular dysfunction. Patients with these ECG patterns should be thoroughly evaluated for congestive heart failure. Patients with LBBB, low ejection fractions, and heart failure are treated with cardiac resynchronization therapy, using a pacemaker that paces the atria and each ventricle, synchronizing both the A-V coupling interval and the depolarization of the ventricles for optimum cardiac output.
REFERENCE: Circulation: Arrhythmia and Electrophysiology. 2008; 1: 127-139 doi: 10.1161/CIRCEP.108.777904
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
LBBB and What Else?
Ken Grauer, MD www.kg-ekgpress.com [email protected]