
Submitted by Dawn on Sat, 01/05/2013 - 19:21
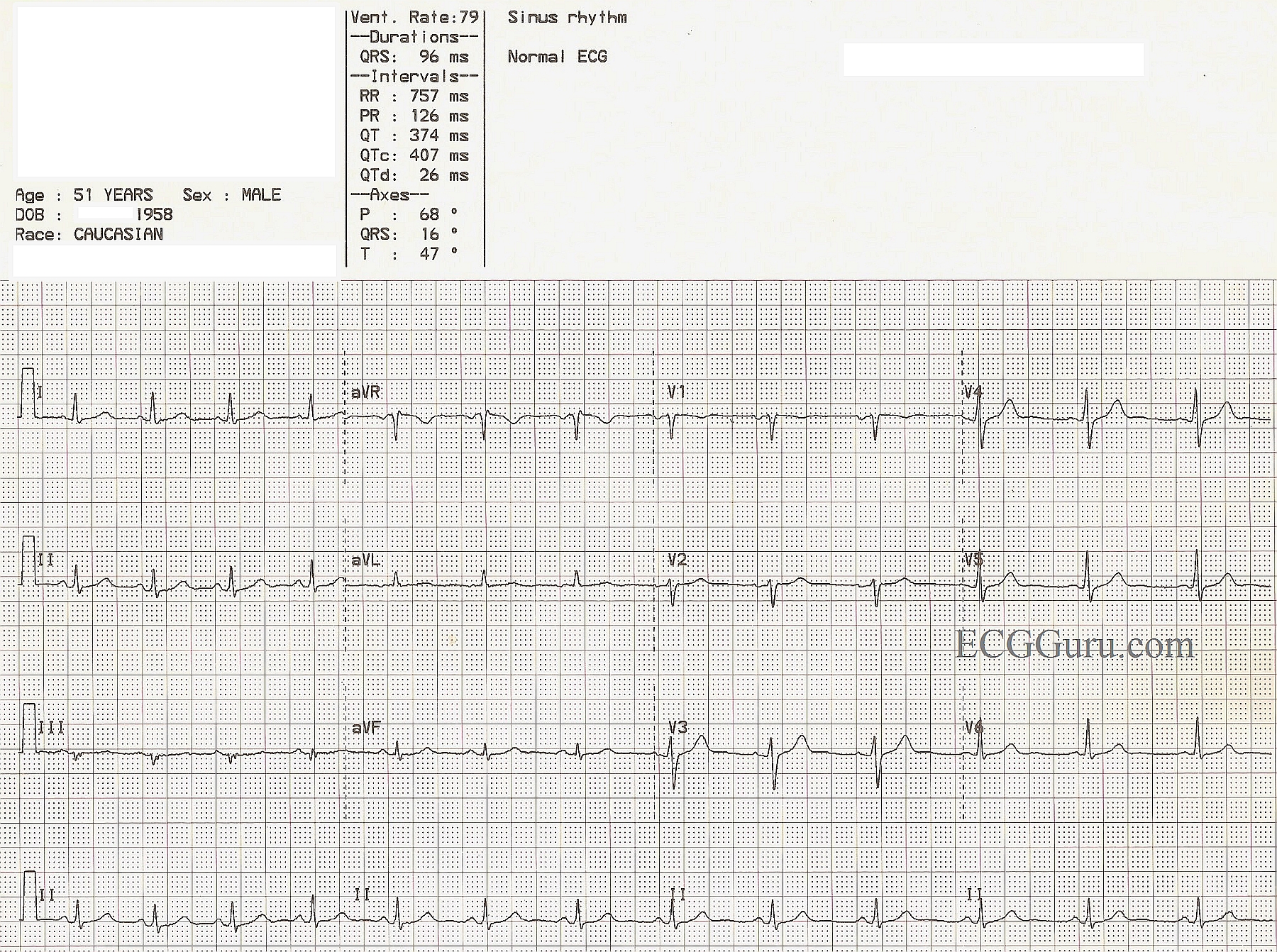
A nice, normal ECG for your collection. It always helps to have a normal ECG for your students to compare to the abnormal examples you show them. It pays to teach the characteristics of "normal" to your students so that they might readily recognize "abnormal". One could argue that the voltage in this ECG is rather low, but that can be explained by body habitus. Whether you are teaching basic rhythm interpretation, axis determination, R wave progression, or intervals, this ECG can be of help to you. Remember, if you are teaching students who have not yet learned 12-lead interpretation, the bottom line of a four-channel ECG is usually a rhythm strip - most often Lead II. It is easy to download this image, then crop it using any photo management program to include only the rhythm strip. At the ECG Guru, we use Irfanview for the Instructors' Collection ECGs.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
When is an ECG "Normal" ?
Amazingly - I sometimes have to look extra hard to find the "normal tracings" in my collection - since many of us who teach get so used to collecting the variety of abnormals that we forget to save enough of the "normals" ... so NICE for Dawn to add a normal tracing for this week's Instructor's Collection. But - is this truly a "normal" tracing ... ?
The Answer is probably YES - but still with a number of "teachable moments" on the tracing. One might take full advantage of these by showing your group the tracing and asking: #1) Is this "normal"?; #2) What aspects of this tracing might be commented on?
I'd answer as follows:
Isn't it interesting to find so much to talk about in a "normal tracing" ?
Ken Grauer, MD www.kg-ekgpress.com [email protected]