
Submitted by Dawn on Sat, 11/24/2012 - 14:52
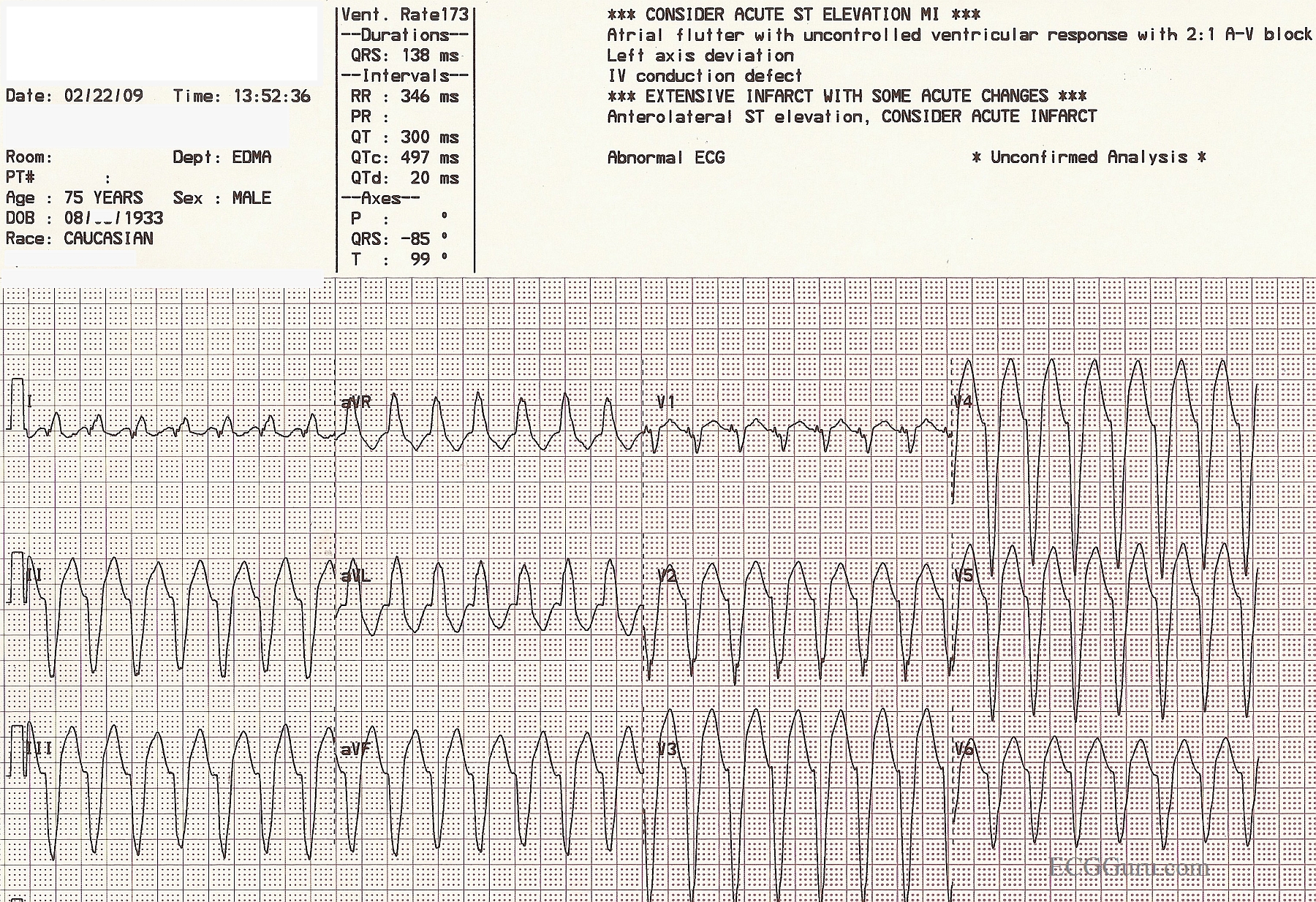
This is a good example of ventricular tachycardia with PRECORDIAL CONCORDANCE. The QRS complexes in the chest, or precordial, leads all point downward. When the precordial leads are all negative or all positive in a wide-complex tachycardia, there is virtually a 100% chance that the WCT is ventricular tachycardia. This ECG shows many characteristics of VT, including the extreme "backwards" axis: aVR is positive and II, III, and aVF are negative. Lead I is almost equiphasic. Also, the lack of a clear BBB pattern and a negative V6 are strongly suggestive of VT. REMEMBER: In the treatment of wide-complex tachycardia, the rhythm should be considered VT unless proven otherwise. This is especially true in unstable patients, patients over 50 years old, and patients with known heart disease.
INSTRUCTORS' NOTE: We purposely left the machine interpretation on this week's ECG of the Week. How many errors did the machine make? This might be a good teaching point for students of all levels.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
POSSS
Just POSs. very SMALL R wave in V1, V1R/V6S
How Many Ways VT?
GREAT illustrative tracing by Dawn. I love her point about the computer interpretation. There are Pros and Cons in using computerized ECG interpretations — but this tracing brings home the point that IF a computerized interpretation ever says anything but "sinus rhythm" — Do NOT believe it! I do not think there will ever be an adequate computerized program for rhythm interpretation (For anyone interested in brief Review on Computerized tracings plus a series of ECGs with answers on "computer mishaps" — CLICK HERE — ).
But the MAIN point about this wonderful example is HOW MANY WAYS YOU CAN DIAGNOSE VT on this tracing. Just count the ways:
FINAL POINT — We can also say 100% that this is NOT WPW — because the QRS in leads V4,5,6 is all negative. This means the impulse arises near the apex — and no accessory pathways originate down there ...
GREAT teaching tracing Dawn!
P.S. For review of the criteria I favor for distinguishing VT vs Aberrancy — Please see my ECG Blog #42 —
Ken Grauer, MD www.kg-ekgpress.com [email protected]