
Submitted by Dawn on Fri, 01/14/2022 - 16:58
The patient: This ECG is from an 87-year-old man who was transported to the Emergency Department by paramedics. His chief complaint, as reported by caregivers, was lethargy, fever, and a declining mental status. He appeared tired and slightly confused, and was normotensive.
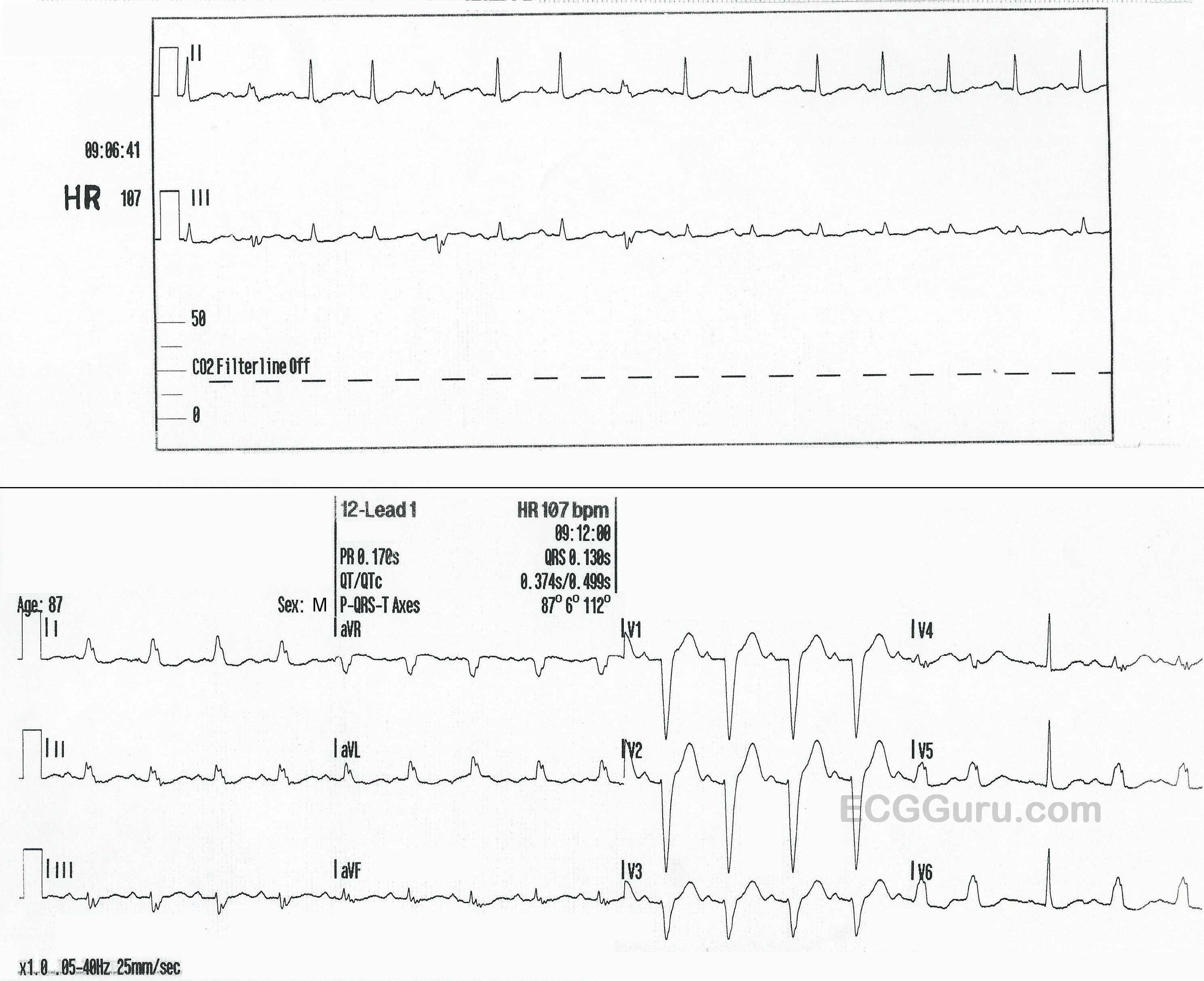
The ECG: There are a rhythm strip with two leads, II and III, and also a standard 12-lead ECG. The RHYTHM STRIP shows a tachycardiac rhythm that slows very slightly toward the end. The rate is around 107 bpm, with an R to R interval of approximately 543 ms in the earlier, regular portion. There are regular P waves present, all followed by QRS complexes. Most of the QRS complexes are normal width, but the 2nd, 5th, and 8th are slightly wide at 130 ms, or .13 seconds.
These wider QRS complexes represent aberrant conduction with LBBB occurring intermittently. Aberrant conduction often occurs due to a faster heart rate, but the only clue here is the intermittent conduction disturbance seems to disappear when the rate slows very slightly. It is hard to determine mechanism of aberrant conduction when we have only a ten-second rhythm strip.
The 12-LEAD ECG has essentially the same rate and rhythm, except all the beats in the first ¾ of the ECG are conducted aberrantly, in a LEFT BUNDLE BRANCH BLOCK pattern. This indicates that the LBB is refractory at this time. Beat No. 15 is premature (PAC). The pause after the PAC allows the left bundle branch to repolarize, conducting one single beat normally.
Conclusion: The patient was determined to be septic, secondary to a urinary tract infection. We do not know his outcome.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Rate-Related vs Intermittent BBB vs Aberrant Conduction
Interesting tracing! I wish resolution was better ... but we CAN see the essentials.
As per Dawn — the 12-lead ECG shows sinus tachycardia @ 107/minute with LBBB except for the 3rd-to-last beat. As Dawn notes — this beat is preceded by an early beat (a PAC) — which produces a slight pause, which is enough to allow the left bundle branch to fully recover conduction properties.
As I explain in detail in my ECG Blog #242 = https://tinyurl.com/KG-Blog-242 — including the 8-minute Audio Pearl on this topic in this post) — true “rate-related BBB” is not common, and it is often challenging to prove. The problem is that the rate of “onset” of the BBB is not necessarily the same as the rate of “offset” — so an extended period of monitoring is often needed to prove this phenomenon. NOT here — because we capture normal conduction immediately after the PAC-induced pause AND because of what we see in the long dual-lead rhythm strip.
It is easy to be disoriented by the rhythm strip — because the “wider” QRS complexes (2nd, 5th and 8th beats) are small — but if you compare QRS morphology of this lead II and lead III rhythm strip — with leads II and III in the 12-lead — QRS morphology is IDENTICAL, proving that conduction for the 2nd, 5th and 8th beats in the rhythm strip IS with LBBB.
The KEY for assessing the rhythm strip — is to verify that P waves remain regular throughout — AND — that the PR interval preceding beats #2, 5 and 8 is IDENTICAL to the PR interval of normally-conducting beats. Therefore — this proves there is intermittent LBBB conduction!
There is great variation in Terminology. My preference ( = my opinion) — is that rather than “aberrant conduction” — what we are seeing in today’s tracing is “rate-related BBB” for the 12-lead — and “intermittent” LBBB for the rhythm strip. TRUE — that both of these are manifestations of a similar phenomenon — but since the “rate” doesn’t change for the rhythm strip — it is not what I think of as “aberration” (that tends to be induced by abnormal conduction due to very early premature impulses). Instead — when there is disease in one of the bundle branches — sometimes you’ll see intermittent conduction (every 2nd - or every 3rd - or every 4th, etc) beat — until over time the patient eventually develops “permanent” BBB with every beat.
TRUE — that you could consider the 12-lead as manifesting “LBBB aberrancy” for all but 1 beat — but I think it clearer ( = my opinion) to simply say there is “rate-related BBB”.
BOTTOM LINE: Clinical implications of complete and permanent BBB (left or right) — and/or of intermittent or rate-related BBB are virtually the same. However, clinical implications of “aberrant conduction” are not necessarily the same, because there may be a physiologic reason for intermittent aberrant conduction (ie, an early PAC occurring at a time when one of the bundle branches is still refractory).
========================
For more on the phenomenon of “rate-related BBB” — Please check out my ECG Blog #242 = https://tinyurl.com/KG-Blog-242 — (including the 8-minute Audio Pearl on this topic in this post).
For more on “my take” of aberrant conduction — Please see Blog #211 = https://tinyurl.com/KG-Blog-211 (including the 5-minute Video Pearl in this post).
Ken Grauer, MD www.kg-ekgpress.com [email protected]
intermittent LBBB not purely frequency-depended
Here is another example of an intermittent LBBB. The p-waves are marked with blue arrows. The LBBB mainly occurs at PACs, but also in SR. Thus this is an intermittent and not purely frequency-dependent LBBB.
Here is another example of an
Here is another example of an intermittent LBBB, in this case frequency-dependent. Excerpts from the stress ECG of a 56-year-old woman with no cardiovascular risk factors and no symptoms, no known previous cardiac disease. The image shows a screenshot when LBBB begins