
Submitted by Dawn on Sun, 06/10/2018 - 13:33
The Patient This ECG was recorded from an 86-year-old man who was weak, pale, and diaphoretic. He was hypotensive, with a BP of 88/54. He denied chest pain or shortness of breath.
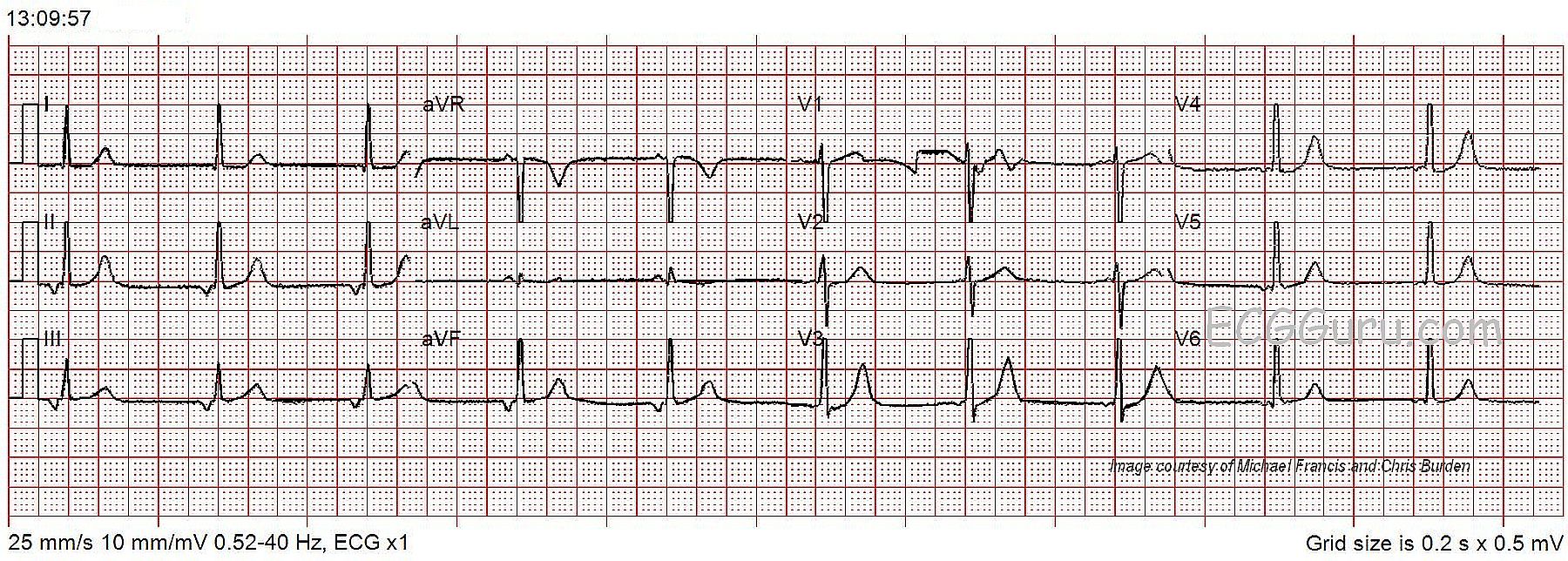
The ECG The 12-lead ECG shows a bradycardia at about 60 beats per minute and regular. The QRS complexes are narrow, at a little less than .08 seconds (800 ms). The P waves are negative in Leads II, III, and aVF and positive in aVR. This is an indication that the P waves are traveling in a “retrograde” fashion – backward. The origin of the P waves has to be the AV junction or the lower atria for this to happen. The PR interval is on the short side of normal at about .12 seconds (120 ms), possibly even less. This is common in junctional rhythm, as the impulse starts at the AV junction, and travels back through the atria and forward through the ventricles at the same time.
There are no premature beats, and the ST segments are not elevated or depressed. There are no T wave inversions, except for aVR, where it is normal.
Assessment One cause of junctional rhythm is sinus brady. That is, the sinus node begins firing so slowly that the junctional pacemaker “escapes”, and takes control of the heart. When the sinus node speeds up, it may once again take over the heart’s rhythm from the junction. The fastest pacemaker controls the heart. A junctional rhythm may escape when the sinus node fails or there is a complete AV block in the AV node area.
Patient Outcome This patient was diagnosed with orthostatic hypotension, bronchitis, and urinary tract infection. He was treated in the hospital and cleared by a cardiologist for discharge two days later.
Our thanks to Michael Francis and Chris Burden for donating this ECG.
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Low Atrial vs Junctional Rhythm in an 86-Year Old
We are told that the patient whose ECG is shown in the Figure is 86 years old — and that he presented with weakness, urinary tract infection, and hypotension with an orthostatic component. As per Dawn — the rhythm is not sinus, because P waves are not upright in lead II. Instead, there are inverted P waves in the inferior leads, with an upright P wave in lead aVL. The rate is ~60/minute. T waves are somewhat peaked in multiple leads, but as per Dawn — there is really no significant ST segment deviation. I’d add the following points.
Ken Grauer, MD www.kg-ekgpress.com [email protected]
Low Atrial v. Junctional
I agree with Dr. Grauer that this most likely represents a low atrial pacemaker. The P'-R interval with a junctional ectopic pacemaker depends on the relative difference in conduction time from the pacemaker site to the atria versus to the ventricle. In this particular case, there would obviously be more delay entering the ventricle than the atrium. But I am going to play the odds here. A low atrial pacemaker generally does not travel via a conduction tract but instead it travels cell-to-cell. Now, cell-to-cell conduction in the atria is not the problem it is in the ventricle because of the thinner walls and the shorter refractory periods. However, no matter how close an ectopic atrial pacemaker site is to the AV node, it is very, very rare for the conduction time to result in a P'-R interval less than 0.12 seconds. It CAN happen, but again, it's very rare. The same goes for the P'-R interval with an ectopic junctional pacemaker. Of course, here the P' and the QRS have no direct connection since they are both the result of a preceding junctional pacemaker discharge. However, it is also very, very rare for the P'-R interval of a junctional beat to be more than about 0.08 seconds (80 msec) - NOT impossible but again, very rare. I think this is a low atrial rhythm.
I'm wondering if the SA node is experiencing a sinus arrest or 3rd degree SA block because there are no sinus P waves anywhere that I can see. However, the ectopic rhythm could be suppressing the SA node by overdrive suppression.
As for the T waves, they are not very impressive, but V3 certainly looks a little too peaked for comfort. Given this patient's age and history, a serum K+ is certainly in order. The classic hyperkalemic T waves only appear about 19% of the time so we often have to depend on our diagnostic and clinical skills and a hefty dose of suspicion!
As far as getting a cardiology consult, I think that is going to depend on one's comfort zone in interpreting ECGs. For us that is not much of an issue, but unfortunately - Ken and Dawn - we still have a lot of work to do educating our colleagues to a higher level of ECG expertise than just a cloudy recollection of what is in Dubin's book. A cardiologist friend of mine says he is still getting calls about acute ischemia that turn out to be nothing more than classic repolarization abnormalities in a chronic bundle branch block.
Thanks Dawn, for posting this ECG and thanks to Michael and Chris for submitting it.
Jerry W. Jones MD FACEP FAAEM
https://www.medicusofhouston.com
Twitter: @jwjmd
Thanks, Drs. Grauer and Jones
Your comments are so helpful in sorting out some of the confusion around ectopic pacemakers - prematurity and escape, low atrial vs. junctional, etc. This one was difficult for me because the PR interval was not VERY short or VERY long. Sometimes, I don't want to commit when things seem borderline. :-D I agree with both of you about wishing there was a higher confidence among physicians and other health care personnel when it comes to ECG. I am an RN, and I was very distressed to find that the topic was barely covered in nursing school, and it seems that things have not improved much in the MANY decades since then! I was not far into my nursing career when I found myself giving basic ECG tests to physicians who were taking ACLS and finding that they did not read common rhythm strips well! I am very glad there are teachers like both of you to continue to set the bar a little higher for the rest of us.
Dawn Altman, Admin