
Submitted by jer5150 on Sat, 09/22/2012 - 12:11
Patient's clinical data:
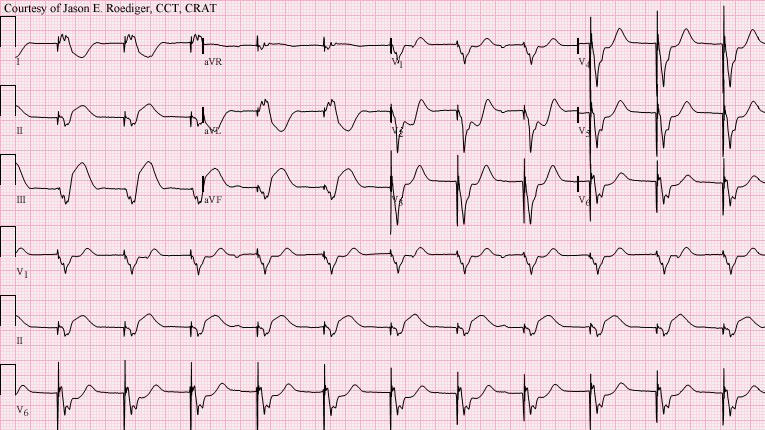
75-year-old white man who presented to the emergency department. The patient was ventricularly paced on an emergent basis and the indication was probable complete AV block with an ineffective junctional escape rhythm. I don't believe this patient survived the admission of this hospital visit.
This is the next-to-last ECG that was performed on this patient. ECGs immediately recorded, just prior to this one, were of such suboptimal quality that I've determined they aren't worthy of posting in this blog. However, you don't need to view them in order to know what non-arrhythmic feature this patient's intrinsic rhythm was showing.
It could easily be argued that if you showed this 12-lead ECG to many healthcare providers, the vast majority of them would probably interpret it as nothing more than "V-paced".
Questions:
(1.) What is obviously "shining through" despite the fact this patient's rhythm is ventricularly paced?
(2.) What eponymous criteria do we use to interpret this ECG?
Rate this content:
-

- jer5150's blog
- Log in or register to post comments
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Inferior Wall MI and CAVB
The striking finding is the ST elevation in the inferior leads. There is reciprocal changes in I, aVL and V1-V3. The rhythm is sinus with CAVB.
V-paced rhythm
Even though V-pacing can cause ST segment elevation that is totally due to the pacing, in this example the magnitude and the shape of the ST elevation in the inferior leads is suggestive of underlying acute injury. V-pacing with the typical electrode postision in the right ventricular apex would not normally cause this shape of ST elevation in these leads.
Inf-Post MI
Inf-Post MI
INTERPRETATION
This patient was having an acute inferior infarction. The criteria that we use for determining this was developed by Dr. Elena B. Sgarbossa (et al.) and has eponymously been referred to as the "Sgarbossa criteria". Dr. Bill Nelson alternately refers to this same criteria as the "Gusto criteria" so named after the GUSTO-1 trial (Global Utilization of Streptokinase and Tissue Plasminogen Activator for Occluded Coronary Arteries). The pacemaker is pacing the apex of the right ventricle (RV) and is probably programmed in a demand mode. There is a dissociated sinus bradycardia at a rate of about 50/min. Below, I have included a wealth of information on this subject matter. Please endulge yourselves in reading up on this very important topic!
Internal links within the ECG Guru website:
(1.) http://www.ekgguru.com/content/paced-rhythm-acute-anterior-lateral-mi
(2.) http://www.ekgguru.com/ecg/lbbb-acute-mi
(3.) http://www.ekgguru.com/content/left-bundle-branch-block-acute-mi-how-much-truth-teach
Sources/References:
(1.) http://xa.yimg.com/kq/groups/10355996/561602581/name/sgarbossapace.pdf
(2.) http://www.columbiamedicine.org/education/r/Cardiology/ACS/Clinical%20Decision-Risk%20Assessment/Sgarbossa%20Criteria.PDF
(3.) http://ems12lead.com/?feb_network_search_context=blog&s=sgarbossa+
(4.) http://lifeinthefastlane.com/ecg-library/basics/sgarbossa/
(5.) http://en.ecgpedia.org/wiki/MI_Diagnosis_in_LBBB_or_paced_rhythm
(6.) http://www.youtube.com/watch?v=9he_lHyn91A
(7.) http://www.cinc.org/archives/2010/pdf/0277.pdf
(8.) http://www.ekginterpretation.com/library/myocardial-infarction-in-the-presence-of-lbbb/
(9.) http://www.emergency-medicine-tutorials.org/Home/medical-3/cardiovascular/ecgs-1/scarbossa-criteria
(10.) https://docs.google.com/viewer?a=v&pid=sites&srcid=ZW1lcmdlbmN5LW1lZGljaW5lLXR1dG9yaWFscy5vcmd8d3d3fGd4OjFjOThmMGQ2NGNiYmY1YjU
(11.) http://ekgumem.tumblr.com/post/53203152998/tombstones-checkmarks-and-bundles-oh-my
(12.) http://ecg.bidmc.harvard.edu/mavendata/images/case24/1350x900.gif
(13.) http://www.ufrgs.br/imunovet/molecular_immunology/EKG_AMI_inferior_LBBB.jpg
(14.) http://hqmeded-ecg.blogspot.com/search?q=Sgarbossa
Jason E. Roediger - Certified Cardiographic Technician (CCT)
[email protected]
Diagnosis
Sinus arrest with ventricular pacemaker VVI mode
Dr. Mostafa Refaat
sinus bradycardia or sinus arrest
Convinced with the rest of the findings but i chouldn't appreciate a very continuos p-wave rhythum. To me underlying rhythum appears more like sinus arrest.
I beleive you'll make it more clear to me and other.
Thankyou.