QUESTION:
Dr. Jones, what advice do you have for teaching ECG beginners?
Today’s expert is Dr. Jerry W. Jones, MD, FACEP, FAAEM
Jerry W. Jones, MD FACEP FAAEM is a diplomate of the American Board of Emergency Medicine who has practiced internal medicine and emergency medicine for 35 years. Dr. Jones has been on the teaching faculties of the University of Oklahoma and The University of Texas Medical Branch in Galveston. He is a published author who has also been featured in the New York Times and the Annals of Emergency Medicine for his work in the developing field of telemedicine. He is also a Fellow of the American College of Emergency Physicians and a Fellow of the American Academy of Emergency Medicine and, in addition, a member of the European Society of Emergency Medicine.
Dr. Jones is the CEO of Medicus of Houston and the principal instructor for the Advanced ECG Interpretation Boot Camp and the Advanced Dysrhythmia Boot Camp.
ANSWER:
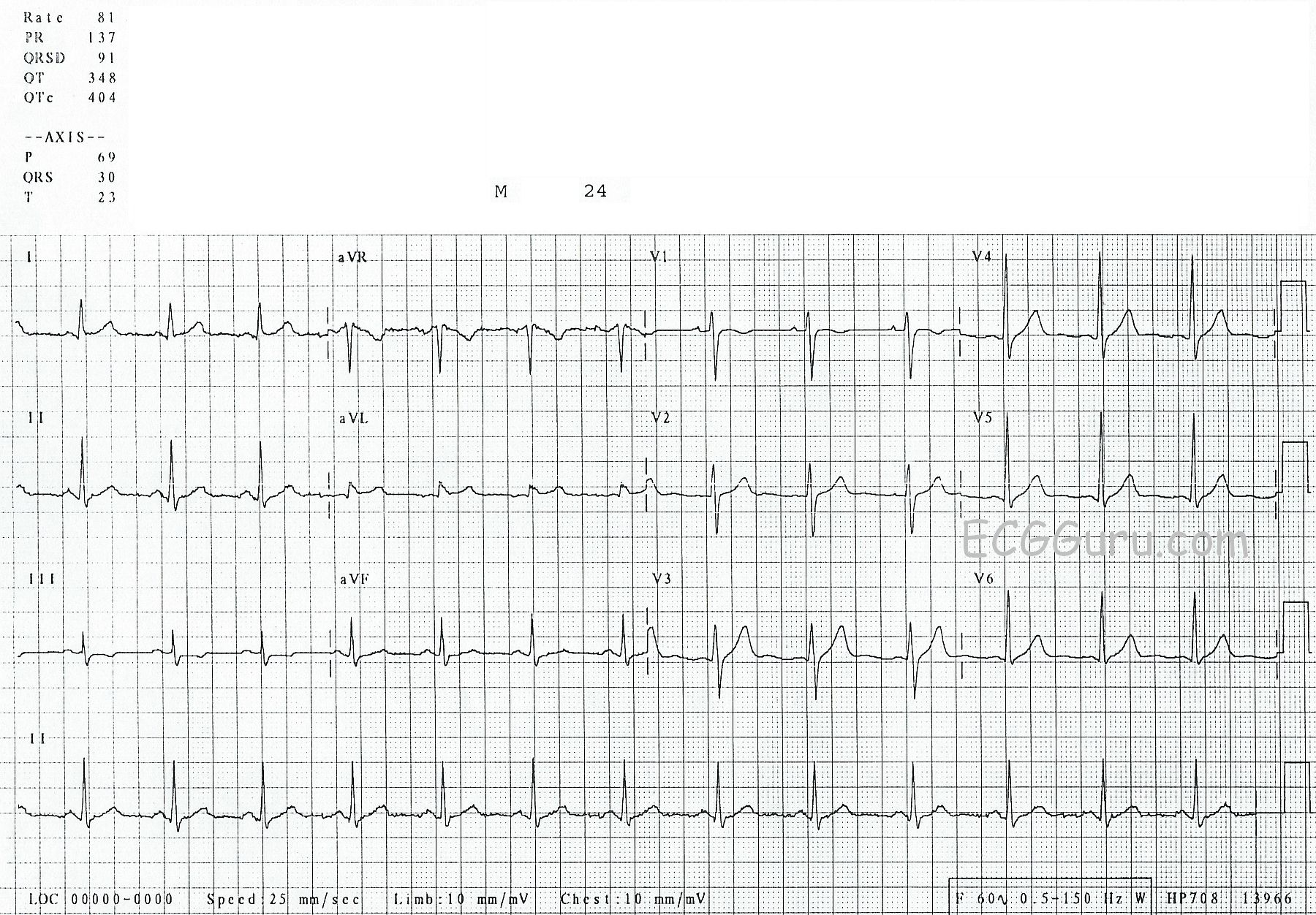
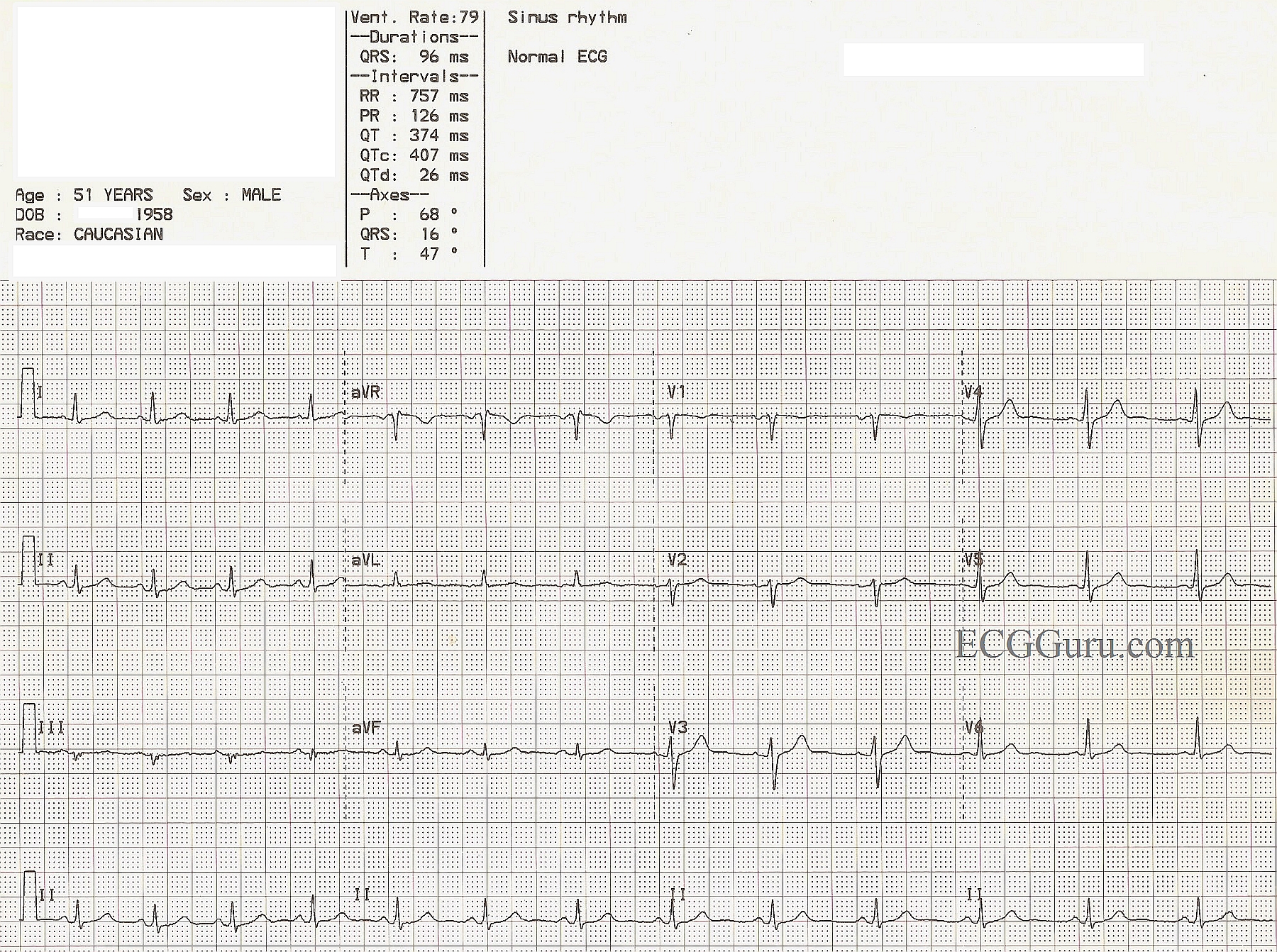
Even in my advanced classes I begin with "normal" ECGs. Throughout my residency in internal medicine, I was never up at 3 am wondering if an ECG was ABNORMAL ... I was always trying to decide if a finding was really NORMAL instead.
Here are a few of my thoughts...
A biphasic P wave in V1 is basically the norm. Even when there is only a monophasic deflection, it's usually because the other half of the biphasic deflection is isoelectric.
In my advanced courses we always begin with a normal tracing and I have all the participants measure the R-R intervals with ECG calipers to demonstrate that there is often considerable variation in the rhythm and that there is very rarely a perfectly regular sinus rhythm (and when there is - it's only for a few moments!). This comes in handy occasionally in deciding whether a tachycardia is sinus or not.
I often find that beginners have the impression that the R waves in the precordial leads increase in size from V1 through V6 - and that should never be the case in a "normal" ECG. Typically the tallest R wave peaks at V4 or V5. Because the V6 electrode is the furthest of all the regular precordial leads from the surface of the heart, it actually diminishes in amplitude. When the R wave in V6 is the tallest across the precordium, it means that the heart has enlarged enough to extend its surface a lot closer to the V6 electrode. That alone is a very good indication of cardiac enlargement.
One other thing I would really emphasize to a newbie is that the ST segment should rise gently into the upslope of the T wave and that there should never be a perceptible angle indicating where the ST ends and the T wave begins - it should be smooth and without a discernible margin. And the T wave should always be asymmetrical - NOT symmetrical. However, when the downslope of the T wave returns to the baseline it CAN create a noticeable angle.
I hope some of these comments help you teach those who are just beginning to read ECGs.