When teaching ECG, I always try to make the ECG interpretation have some practical context for the student. Why study squiggly lines, if they don't mean something to our care of our patients? Even putting a simple scenario (actual or invented) with an ECG can make it more relevant for your students. A series of ECGs taken as the patient undergoes changes, is especially helpful.
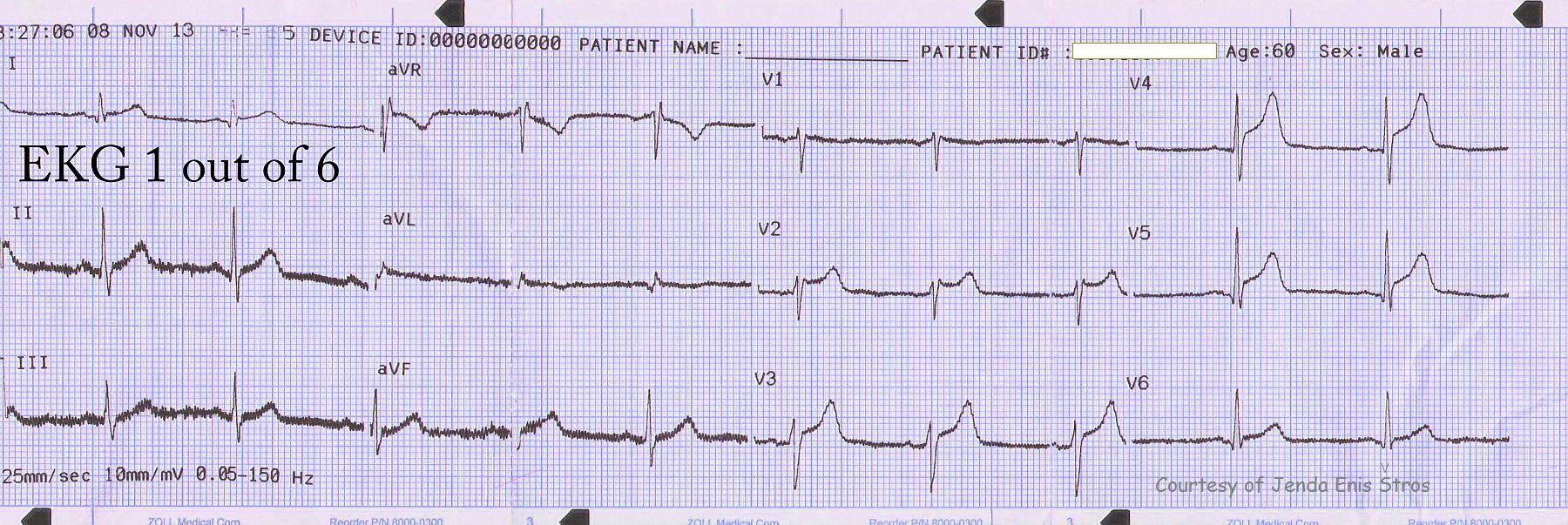
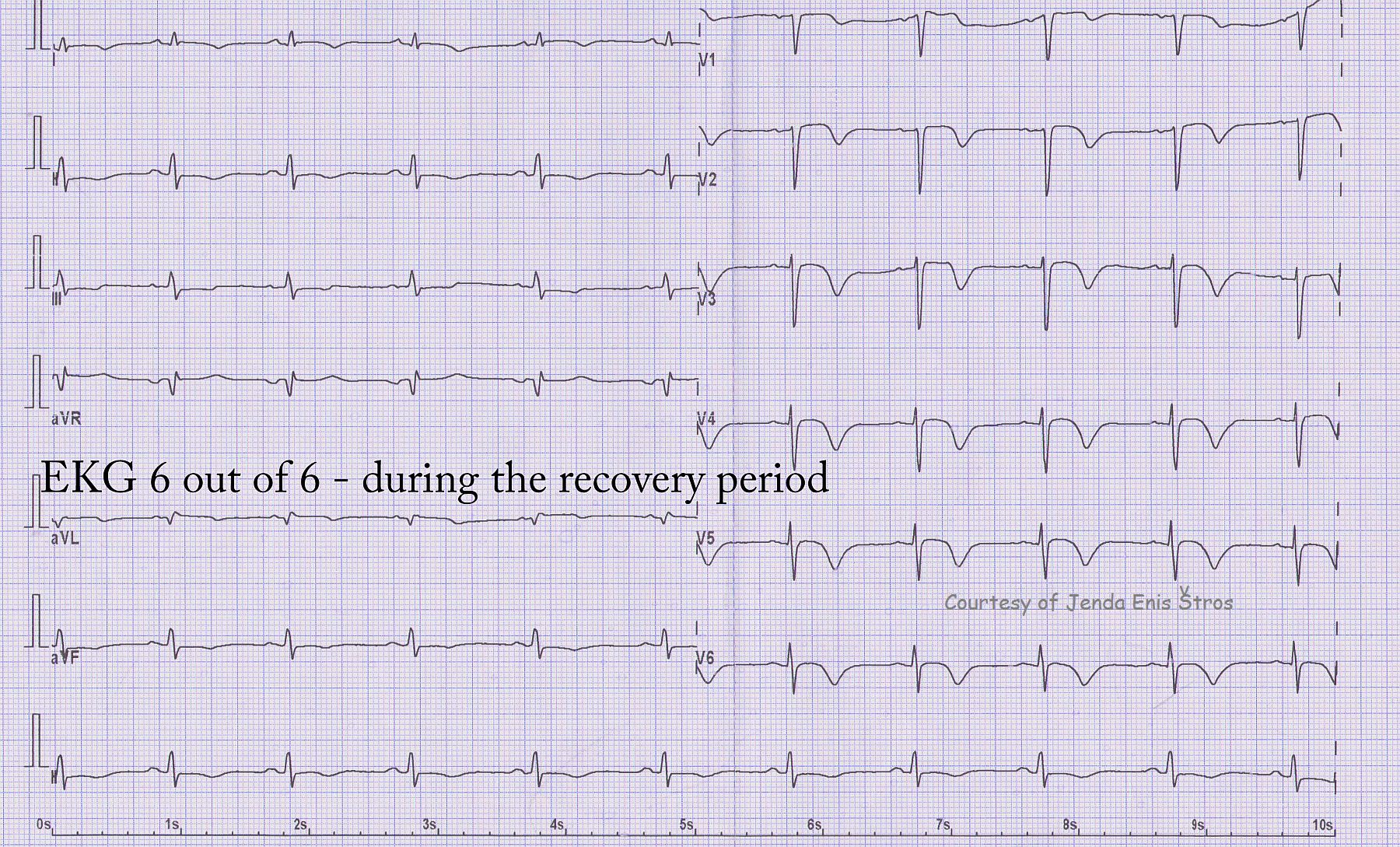
This ECG is the last in a series of 6 that were donated by Jenda Enis Štros showing the evolutionary changes of an M.I. from onset, through spontaneous reperfusion, angioplasty, re-occlusion by thrombus, and recovery. This ECG shows deep precordial T wave inversions, an expected evolutionary change after reperfusion of an occluded artery - in this case, the left anterior descending. The patient has lost some of his QRS amplitude (viable heart muscle), but has not developed pathological Q waves. Pathological Q waves would indicate full-thickness necrosis of the wall, which is usually a permanent injury.
The patient was discharged home with a 45% ejection fraction (60% is ideal), and he had akinesis of part of his anterior wall. This can be permanent or temporary, and followup studies would be needed to evaluate the ongoing health and function of the left ventricle.