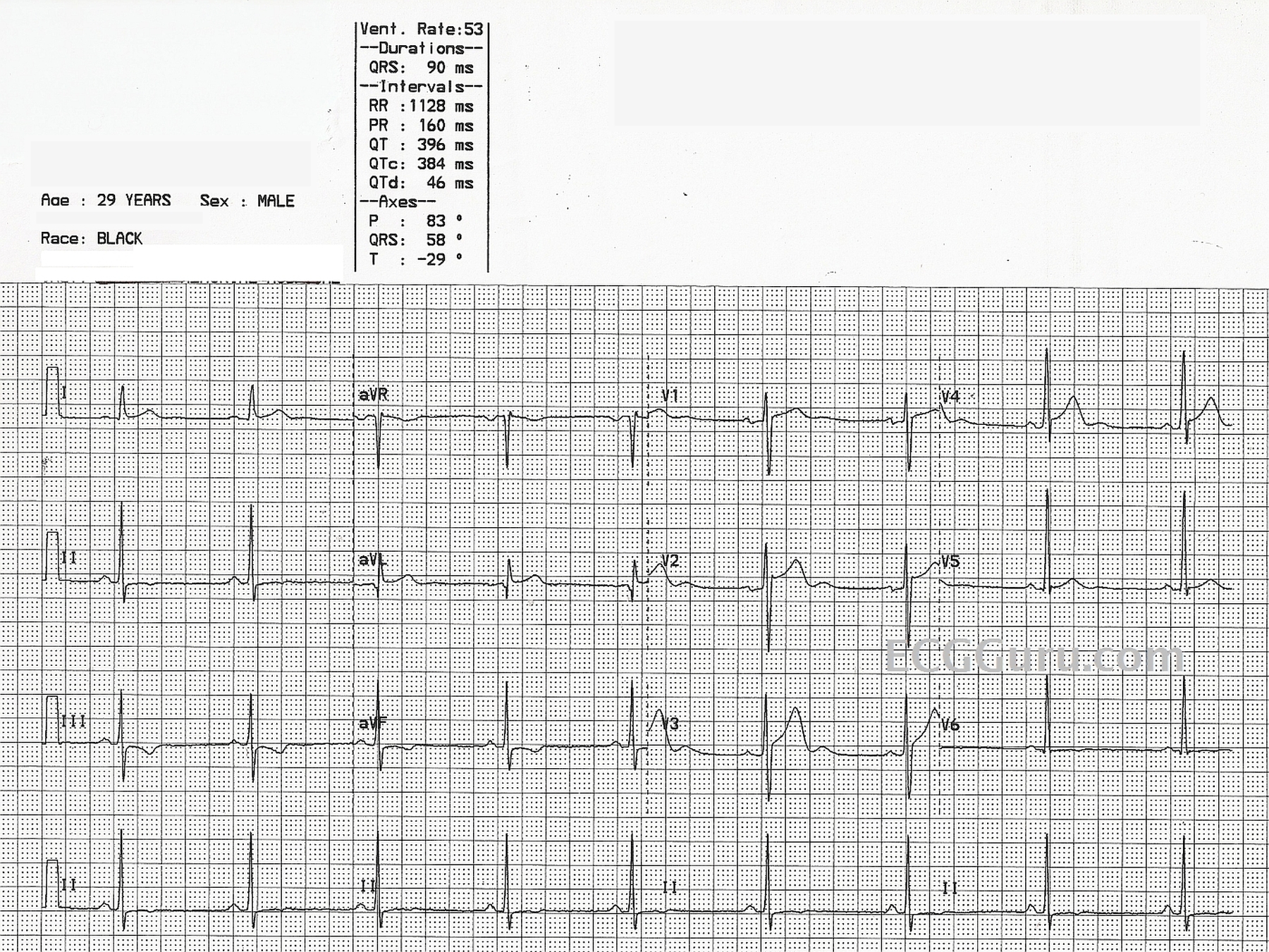
This ECG was obtained from a healthy 29-year-old man. It shows "benign early repolarization". It demonstrates the typical pattern of widespread ST elevation with a normal concave upward sloped ST segment. There are also prominent U waves in V2 through V4, and T wave inversions in the inferior wall leads. He was not complaining of any symptoms and, in fact, donated this ECG as an example of known early repolarization pattern. The other changes may represent normal variations for his age and gender. Early repolarization has long been thought to be a completely benign variant, and it is quite common in young people, especially athletic men. But new research suggests a possible link to future serious arrhythmias. For a discussion of research on this topic from the Journal of the American College of Cardiology, see this link. Research reported in the New England Journal of Medicine can be accessed at this link.
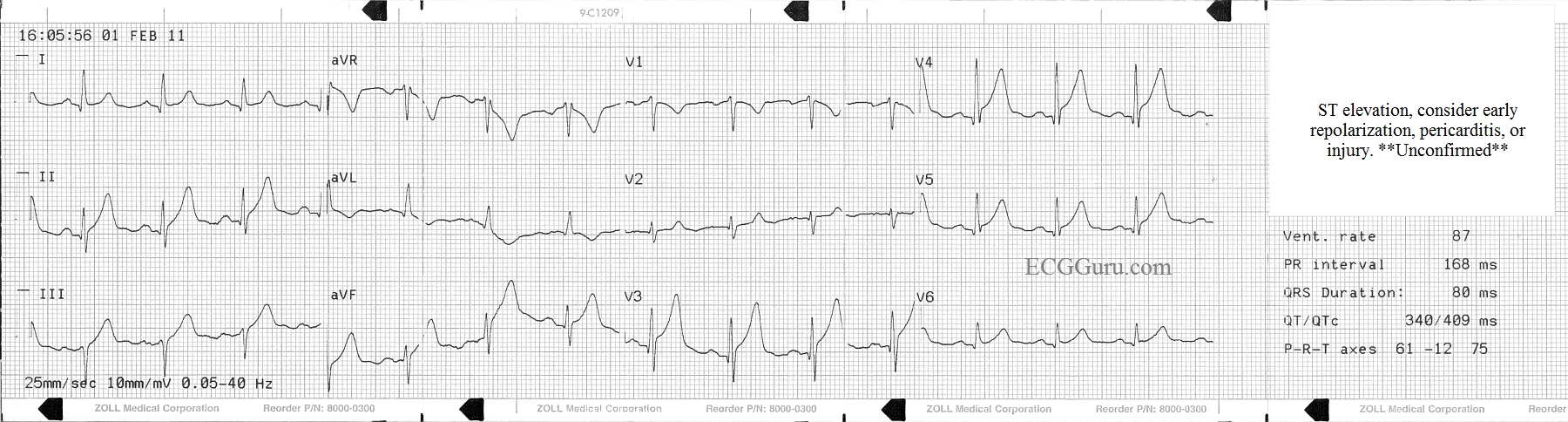
This ECG was obtained from an elderly man who was complaining of acute-onset chest pain, radiating down his left arm. He also complained of a cough, and had audible rhonchi. The machine interpretation gives several possible explanations for the widespread ST elevation noted on the ECG. The paramedics were a bit distracted by the machine's interpretation, and by the respiratory symptoms, and decided not to call a "cardiac alert" on the patient. They did, however, quickly transport him to the closest hospital, which happened to have full-service cardiac facilities. The patient was diagnosed with an acute M.I. and treated with angioplasty in the cath lab, with a good outcome. Afterward, the medics felt that they "overthought" this one, and should have given more weight to the patient's symptoms. Teach your students to evaluate their experiences with open minds and unafraid of self-criticism, so they may learn from every patient. This patient received excellent care, and the paramedics added to their "information banks", upon which they will draw for many years to come.
Although the angiogram results are not available to us, it is plausible that a proximal occlusion of the LCA, near the bifurcation of the LAD and the diagonal, could cause ST elevation in V3 through V6, with mild elevation in Lead II (which is oriented to the leftward portion of the inferior wall), and ST and T changes in the high lateral leads (I and aVL).
Our expert today is Dr. Ken Grauer, M.D., a frequent contributer to the ECG Guru.
KEN GRAUER, MD is ProfessorEmeritus (Dept. Community Health/Family Medicine, College of Medicine, University of Florida in Gainesville). Dr. Grauer has been a leading family physician educator for over 30 years. During that time he has published (as principal author) more than 10 books and numerous study aids on the topics of ECG interpretation, cardiac arrhythmias, and ACLS (including an ongoing Educational ECG Blog).