
Submitted by Dawn on Fri, 07/26/2013 - 16:03
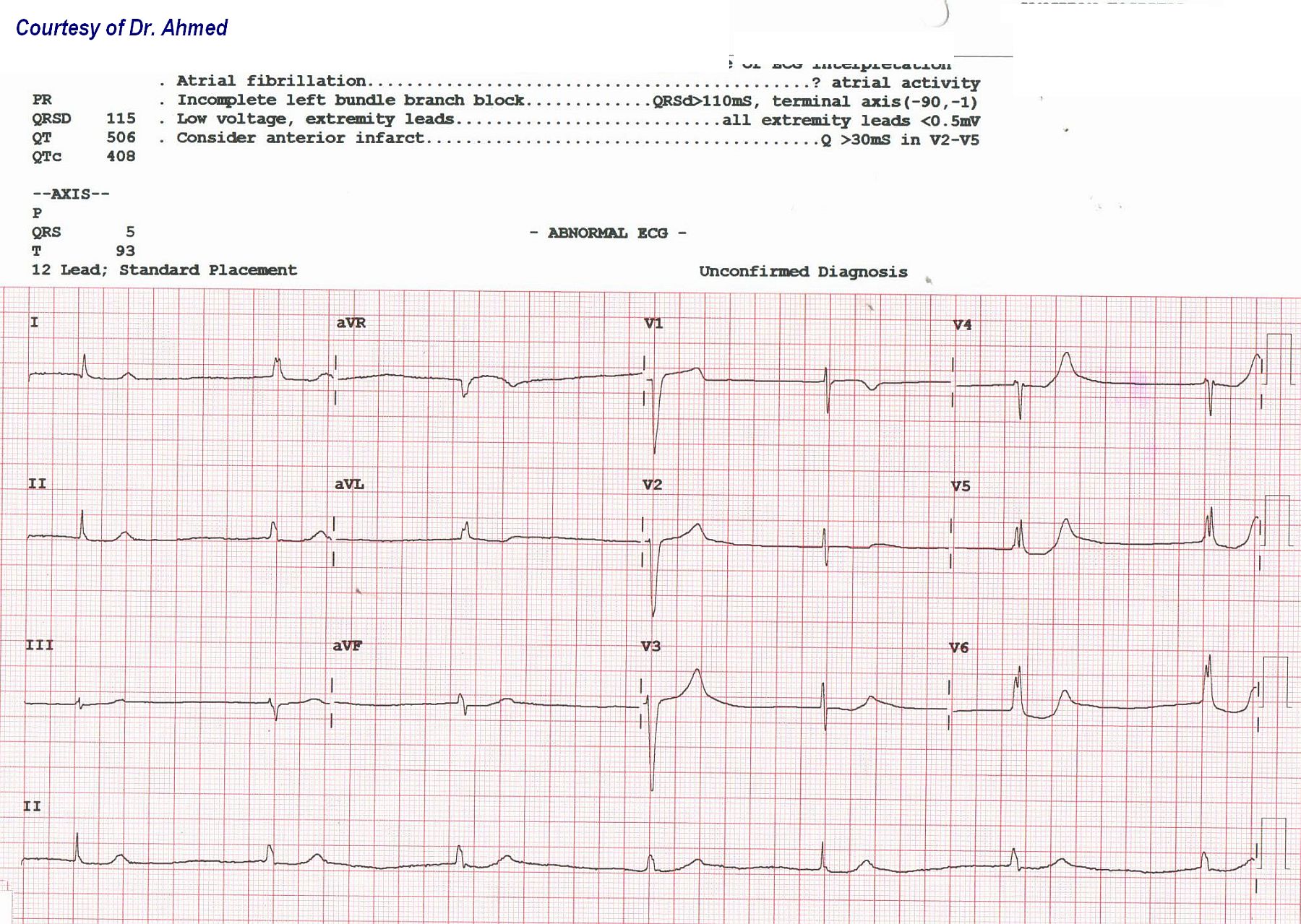
This ECG was kindly donated to the ECG Guru website by Dr. Ahmed for open discussion among our members. The patient was a 70+ year-old man who presented with a complaint of dizziness. His serum potassium level was found to be 6.5 (normal is 3.5 - 5.0). Upon correction of his K levels, his rhythm was atrial fibrillation at 130 / min.
WHAT DO YOU THINK ABOUT THIS INITIAL ECG? What is causing the slow rate? Is there atrial activity? Do you see QRS morphology changes? What about the anterior ST and T wave changes?
We look forward to hearing from our members! And thanks to Dr. Ahmed for donating this interesting ECG.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
AF- hyperkalaemia
Not convinced this is AF. Appears to be P waves immediately after the QRS, even the ectopic beats, at least in the inferior and lateral leads. Appears to me to be a junctional rhythm with supra ventricular ectopics - 1st and 5th QRS complexes. Not quite sure but potentially p waves hidden in the end of these also. Certainly meets criteria for hyperkalaemia, with the broad QRS, and the T waves in the pre cordial leads. Agree with incomplete LBBB.
Slow rate perfectly fits with a junctional rhythm with abberancy in the 1st and 5th beat. Anterior ST, T wave changes consistant with hyperkalaemia. Note the ST elevation in V1? And significant ST depression in low lateral leads (V5 & V6).
What was his K+ after correction? Was it corrected too quickly to cause AF with RVR??? Does he have a history of AF?
Not sure how correct I am with this interpretation, so am certainly keen to hear what others think.
Dual Escape vs SinoVentricular Rhythm in a Hyperkalemic Patient
We are told the patient has hyperkalemia - and it is probable that much of what we see is the result of his K+ = 6.5 mEq/L. Hyper-K+ may cause bradycardia and escape rhythms. P wave amplitude is reduced. Sinoventricular rhythm may occur - in which the P wave disappears from the surface ECG, even though sinus-initiated impulses continue to occur. This may be what we see here - as there are no P waves to be seen.
There are two types of QRS complexes in this ECG: i) a slightly widened QRS (for beats #2,3,4 and #6,7); and ii) a narrow QRS (for beats #1 and #5).
Additional Clinical NOTES:
BOTTOM LINE: A very interesting tracing with dual escape rhythms vs sinoventricular rhythm in a patient with hyperkalemia. I don't believe much more can be said without seeing the ECG after correction of hyperkalemia.
Ken Grauer, MD www.kg-ekgpress.com [email protected]
Test Subject from app
Test