
Submitted by jer5150 on Sat, 12/22/2012 - 11:25
This week, in addition to my own blog, I'm going to feature a guest case study by Guru member Vince DiGiulio, EMT-CC. This past Monday, Vince messaged me (along with Dr. Ken Grauer) on Facebook and requested my input and opinion on these serial ECGs. With Vince's blessing, he gave me permission to use any of his original 12-lead ECGs here on the Guru. Of his 6 ECGs, I've decided to post 4 of them here.
PATIENT'S CLINICAL DATA: 79-year-old female presents to triage with a chief complaint of intermittent dizziness for two weeks that has become rather constant over the past two days. Her pulse is noted to be 38/min and blood pressure 162/84 mmHg. She denies any chest pain or shortness of breath, and has not experienced any syncopal episodes.
QUESTION:
(1.) What's her rhythm?
(2.) What, if anything, did the computer interpret correctly?
Rate this content:
-

- jer5150's blog
- Log in or register to post comments
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
high grade AV block
I think I would decribe this as sinus rhythm with high grade (advanced) AV block and a mixture of junctional escape and capture beats. In the top ECG, QRS complexes 1,3, 5 and 6 are all conducted (capture) beats; the others are junctional escapes. This may be an example of what I think Marriott described as RP-dependent conduction, where an atrial impulse conducts only if it occurs long enough after the previous ventricular depolarisation. However, if this is the case, then the last QRS shouldn't really be a conducted beat, although it certainly looks like one, albeit with aberrant conduction. Could this be an example of supernormal conduction?
The 2nd-from-top ECG is an example of escape-capture bigeminy. There are alternating long and short(er) RR intervals. The long intervals are terminated by junctional esacapes; the shorter intervals are terminated by conducted beats. Most of the P waves are not conducted.
I think the 3rd ECG simply shows complete heart block with a junctional escape rhythm.
The PR intervals in ECG 4 appear constant, so I suspect this is 3:1 AV block.
What did the computer get right? Computers usually struggle with complex arrhythmias such as these, but I would agree with its statement 'Abnormal ECG'! I think it was also right with the ECG it described as showing 3rd degree AV block.
Dave R
INTERPRETATION
I hope I'm not blowing his cover, but I wanted to take this opportunity to acknowledge Dave Richley who is an elected member of the council for The Society for Cardiological Science and Technology (SCST). They are essentially the equivalent of the American Heart Association (AHA) but on the "other side of the pond". We are honored to have him as a member! He is obviously a "Guru" in his own right!
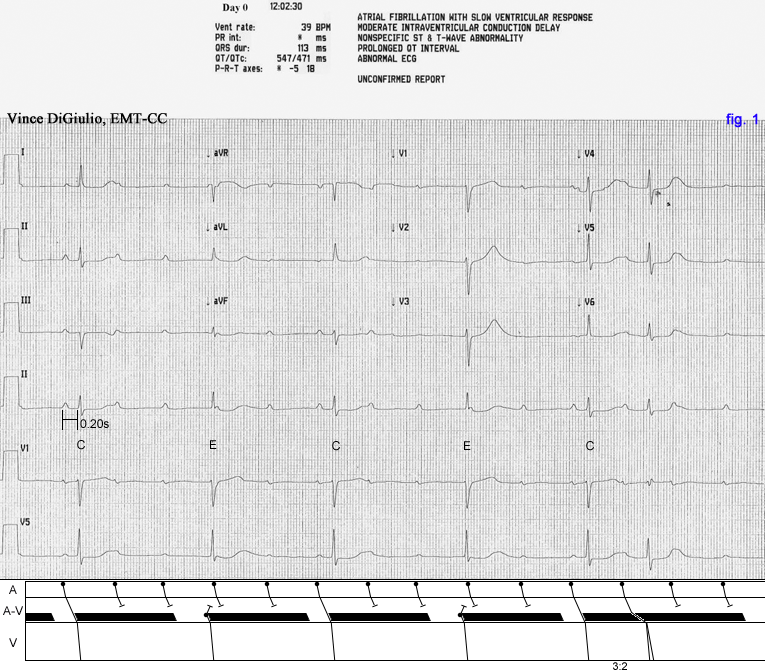
The beats labeled "C" are Ventricular Capture Beats and the beats labeled "E" are Junctional Escape Beats. The junctional escape beats are conducting with what Dr. Marriott called "Type B aberration". Type B aberrancy is loosely defined as an eccentrically-placed junctional focus.
Fig. 1 is probably showing supernormal conduction. I don't think there's any logical way to explain it otherwise. The supernormally conducted beat (6th beat) is additionally conducting with mild incomplete RBBB aberration. In all of the ECGs, I've illustrated the profoundly long absolute refractory period (ARP) as the black-shaded area in the A-V tier. At a critically long R-P interval, successful A-V conduction is possible. This is definitely high-grade since there are two consecutive "dropped" beats due entirely to the A-V block and NOT due to interference from the junctional escape beats. On 3 of the 4 ECGs, the conducted sinus beats all show a borderline or marginally prolonged P-R interval of 0.20s to 0.21s.
Regarding the computer's interpretation: Obviously this is not atrial fibrillation nor is the QRS interval as wide as the computer is calculating it.
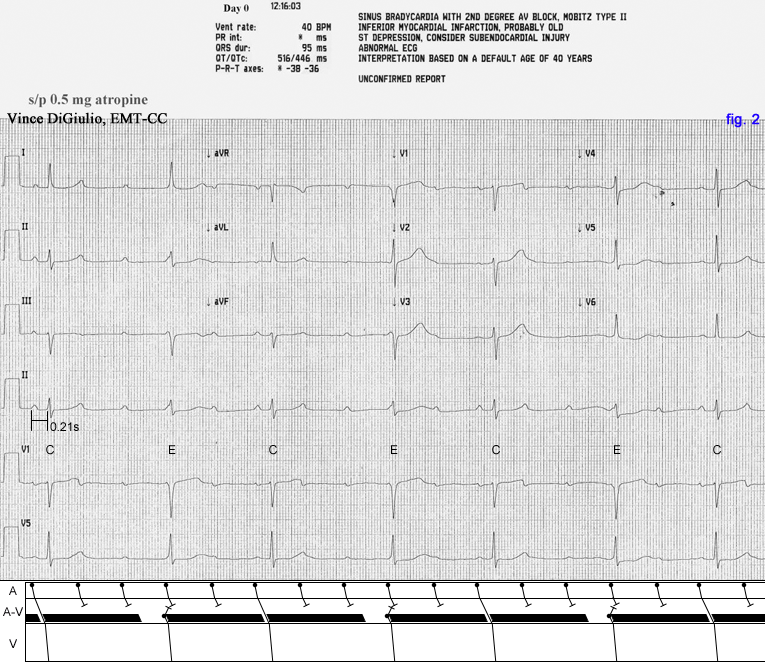
Fig. 2 is showing a manifestation of "Escape-Capture Bigeminy". There is a bigeminal pattern/rhythm with the beats grouped in pairs. The first beat in each pair is a junctional escape (E) beat. The second beat in each pair is a capture (C) beat.
Regarding the computer's interpretation: This is not sinus bradycardia, but rather it is sinus rhythm bordering on sinus tachycardia (i.e., 100/min). As is, I don't think you can speculate whether or not this is a manifestation of Type I or Type II A-V block but it's unquestionably high-grade (advanced) A-V block.
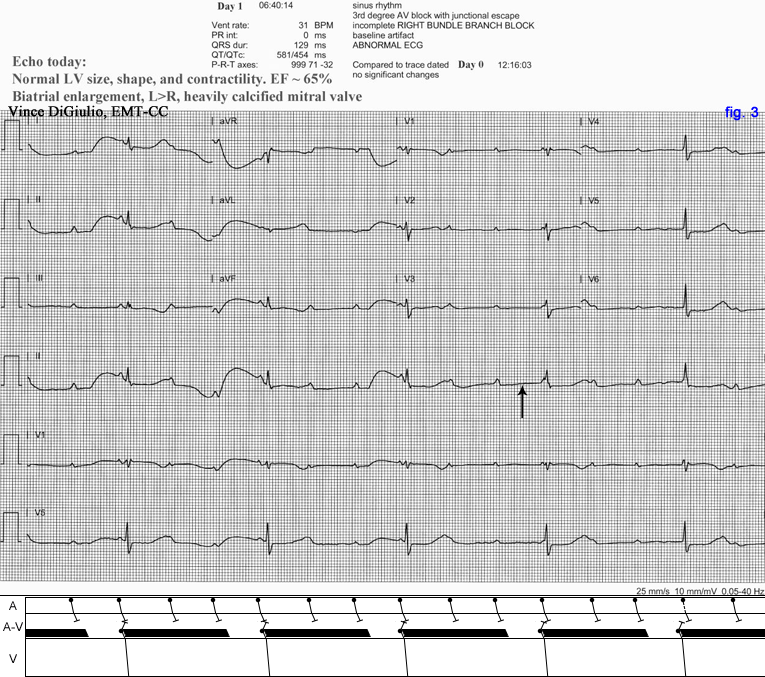
Fig. 3 is showing a potential 3:1 high-grade A-V block with a resulting "passive" idiojunctional escape rhythm. The conductible interval is exceeding the cycle of the junctional escape pacemaker. If a sinus impulse landed exactly where the vertical arrow is pointed, then successful A-V conduction would undoubtedly take place. You can only declare Complete A-V block if atrial impulses probe all phases of the R-to-R interval and conduction still does not take place. From beat to beat, that area of the R-to-R interval where the arrow is pointed is never challenged by an atrial impulse. I would predict that if we were able to view a longer version of this tracing, then there would eventually be a capture beat at a critically long R-P interval thus proving that the A-V block is not complete.
Regarding the computer's interpretation: This may well be a representation of complete A-V block but, as is, I don't think one can prove it.
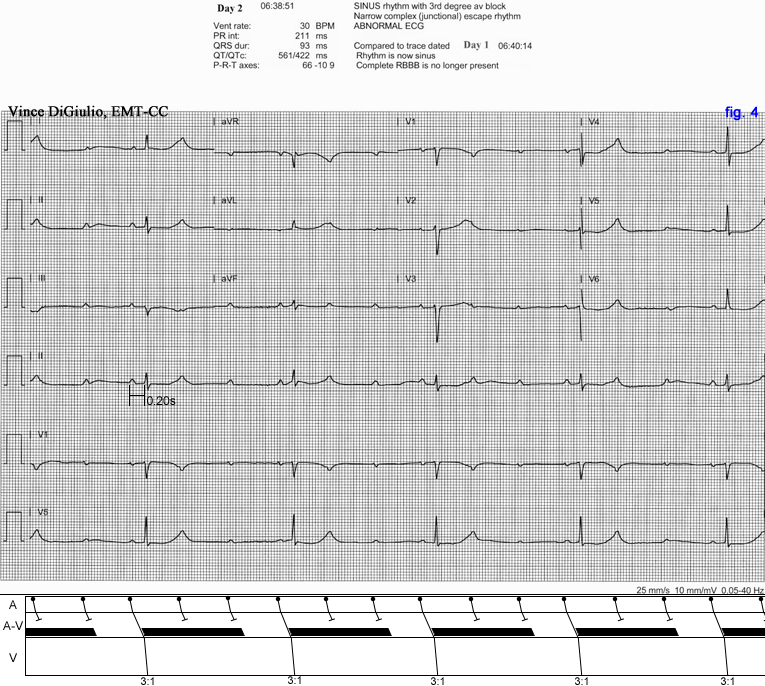
Fig. 4 is just showing a straightforward 3:1 high-grade A-V block.
Regarding the computer's interpretation: Again, this is not complete A-V block since the P-R intervals on the conducted beats are all identical. It's strange that the computer would give a value for the P-R interval if it truely thought that there was no conduction taking place. Note that it did not calculate a P-R interval for Fig. 3.
Jason E. Roediger - Certified Cardiographic Technician (CCT)
[email protected]