
Submitted by Dawn on Thu, 10/27/2016 - 15:33
Question:
Dr. Jones,
I am confused about the repolarization abnormalities that occur in conditions other than acute M.I. (Bundle branch block and hypertrophy, for example). I have been taught that the repolarization abnormalities should point opposite the MAIN part of the QRS, but also I have been told that they should point opposite the TERMINAL deflection of the QRS. Which is right?
Today’s expert is Dr. Jerry W. Jones, MD, FACEP, FAAEM
Jerry W. Jones, MD FACEP FAAEM is a diplomate of the American Board of Emergency Medicine who has practiced internal medicine and emergency medicine for 35 years. Dr. Jones has been on the teaching faculties of the University of Oklahoma and The University of Texas Medical Branch in Galveston. He is a published author who has also been featured in the New York Times and the Annals of Emergency Medicine for his work in the developing field of telemedicine. He is also a Fellow of the American College of Emergency Physicians and a Fellow of the American Academy of Emergency Medicine and, in addition, a member of the European Society of Emergency Medicine. Dr. Jones is the CEO of Medicus of Houston and the principal instructor for the Advanced ECG Interpretation Boot Camp and the Advanced Dysrhythmia Boot Camp.

Answer:
Which Direction Should the Repolarization Abnormality Point?
OK. You've got an abnormal QRS complex followed by a repolarization abnormality (RA). Which direction should the repolarization abnormality point? As a young resident, I was taught that the RA should point in the direction opposite the terminal deflection of the QRS complex. But years later, I see other physicians stating that the repolarization abnormality should point opposite the main deflection of the QRS complex. Which is correct?
The answer is both are correct. Why? How?
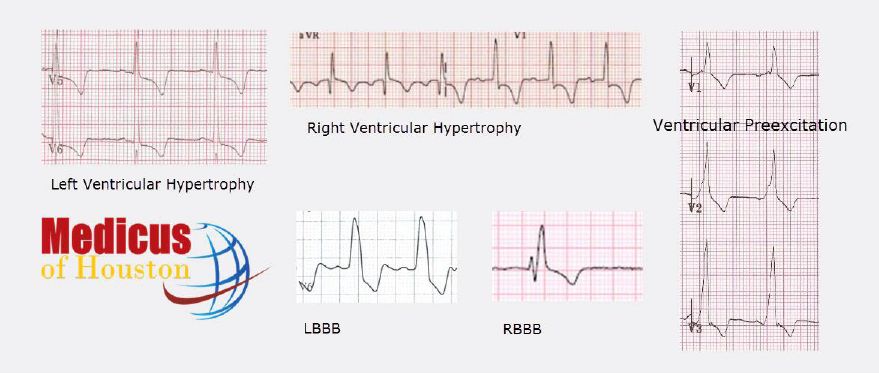
The reason is that the repolarization abnormality is connected to the ventricle in which the problem is located - not the QRS complex itself. To better understand this, let's look at some of the major causes of repolarization abnormalities (you can find examples in the illustration at the top of this page):
Right Bundle Branch Block (RBBB) - When you look at the QRS complex in V1, you see an R and an R'. The R represents left ventricular activation while the R' represents right ventricular activation. So, the problem lies in the right ventricle represented by the R'. The repolarization abnormality reflects the problem in the RV so it should be opposite the R' which is always the last deflection in V1 in the presence of RBBB. Therefore, in cases of RBBB, the repolarization abnormality is always opposite the terminal deflection of the QRS.
Left Bundle Branch Block (LBBB) - When you look at the QRS complex from V6 which has a LBBB, we see a relatively tall, upright monophasic QRS complex. Part of that QRS represents right ventricular depolarization and part represents left ventricular depolarization. But how much of which? We don't know, but all we need to know is that this is a monophasic complex and it is upright. Therefore, since the repolarization abnormality reflects the problem in the left ventricle, and the LV is represented somewhere in that monophasic R, the repolarization abnormality should be opposite the main deflection. Therefore, in cases of LBBB, the repolarization abnormality is always opposite the main deflection of the QRS.
Left Ventricular Hypertrophy (LVH) - When you look at the QRS complexes from V5 and V6, we see a relatively tall, upright monophasic QRS complex. Part of that QRS represents right ventricular depolarization and part represents left ventricular depolarization. But how much of which? Again, we don't know, but all we need to know is that this is a monophasic complex and it is upright. Therefore, since the repolarization abnormality reflects the problem in the left ventricle, and the LV is represented somewhere in that monophasic R, the repolarization abnormality should be opposite the main deflection. Therefore, in cases of LVH, the repolarization abnormality is always opposite the main deflection of the QRS.
Right Ventricular Hypertrophy (RVH) - The same concept discussed regarding LVH applies in cases of RVH. Therefore, in cases of RVH, the repolarization abnormality is always opposite the main deflection of the QRS.
Ventricular Pre-excitation - Most people reading ECGs don't realize that ventricular pre-excitation can also produce a repolarization abnormality. Just as repolarization abnormalities are not always present in cases of LVH and RVH, they are not always present in cases of ventricular pre-excitation, either. However, the repolarization abnormality IS present in some cases. The RA is connected to the ventricle containing the accessory pathway, but don't worry: you don't have to determine which ventricle that is. If a repolarization abnormality is present in a lead, it should be negative if the delta wave is positive and vice versa. Therefore, the repolarization abnormality points opposite to the direction of the delta wave.
So, the question really isn't whether the repolarization abnormality should be opposite the terminal or the main deflection of the QRS. It should be opposite the deflection that represents the involved ventricle.
Related Terms:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
A-Fib Question
Dear Dr.Jones,
my mother in law has A-fib and had a pacemaker put in a few months back, but still has epsoides of her gooing into A-Fib and Taching, is there anyway to really control this, and does the pacemaker really help this problem? She also takes medication, but still has A-fib with heart rate reaching 160 at times. She's 76 years old
thanks,
bob
robert pleasant
Hello, Bob,
I am just seeing this question, sorry. I am answering for Dr. Jones. At the ECG Guru, we are not able to answer your questions about your own health care, or that of your family members. This should be left to the care providers who have knowledge of all the multifaceted aspects of each patient's situation. To try to help clarify one part of your question, however, the pacemaker does not treat the atrial fibrillation. Rather, it protects from loss of rhythm or rate due to the necessary efforts to slow or stop the fibrillation.
Thank you you for your interest in the ECG Guru.
Dawn
Dawn Altman, Admin