
Submitted by Dawn on Wed, 06/15/2016 - 00:57

Question:
Dr. Jones, can you help me understand refractory periods better? I find that a difficult topic to teach, and there are so many different terms used to describe refractory periods.
Today’s expert is Dr. Jerry W. Jones, MD, FACEP, FAAEM
Jerry W. Jones, MD FACEP FAAEM is a diplomate of the American Board of Emergency Medicine who has practiced internal medicine and emergency medicine for 35 years. Dr. Jones has been on the teaching faculties of the University of Oklahoma and The University of Texas Medical Branch in Galveston. He is a published author who has also been featured in the New York Times and the Annals of Emergency Medicine for his work in the developing field of telemedicine. He is also a Fellow of the American College of Emergency Physicians and a Fellow of the American Academy of Emergency Medicine and, in addition, a member of the European Society of Emergency Medicine.
Dr. Jones is the CEO of Medicus of Houston and the principal instructor for the Advanced ECG Interpretation Boot Camp and the Advanced Dysrhythmia Boot Camp.
Answer:
Refractory Periods: Absolute/Relative and Effective/Functional
If you do any reading of the vast amount of literature regarding ECG interpretation, you have certainly encountered the terms effective refractory period and functional refractory period. In introductory courses, we learn about the absolute refractory period and the relative refractory period, but no one ever teaches the effective and functional refractory periods. Most definitions are confusing and incomplete, so I have written a short monograph on this topic.
The effective refractory period is basically the same as the absolute refractory period – but there is a slight difference!
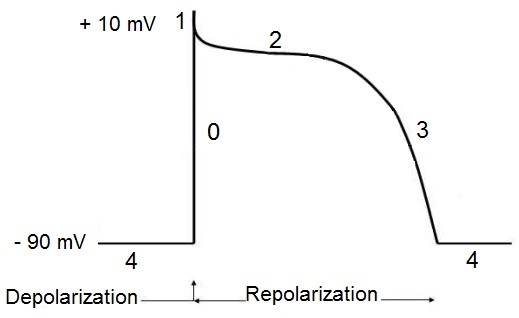
The absolute refractory period is a physiologic state – it begins with the onset of the action potential at Phase 0 and represents the period involving all of depolarization and that part of repolarization during which no amount of stimulus can result in another action potential.
The effective refractory period tries to define the absolute refractory period in more realistic, practical terms. The effective refractory period also represents the period during which a typical impulse cannot produce another action potential. So how does this differ from the absolute refractory period? To understand this, we must now jump to a better understanding of the relative refractory period.
The relative refractory period begins at the point that a maximal stimulus is able to initiate another action potential. The key phrase here is maximal stimulus. If a maximal stimulus occurs one-millionth of one millisecond after the end of the absolute refractory period, another action potential will be generated. But for that action potential to occur, that stimulus will have to be at its maximum amplitude because the threshold potential will be much closer to zero potential than it usually is, thus requiring much greater amplitude to initiate the action potential.
But most Phase 0 depolarizations do not result in maximal voltage. Many times, the arriving impulse does not have a full complement of sodium channels to open, so even though the “all-or-nothing” threshold is reached and an action potential is generated, that action potential has less-than-maximal amplitude. When that is the case, the impulse will have to occur further and further into the relative refractory period before threshold is reached and an action potential is generated. So while there is most definitely an absolute refractory period with a definite end to it, as far as an individual patient is concerned, the “absolute refractory period” may not end until some point well into the relative refractory period. So, for that patient, his/her effective refractory period may be a bit longer than the actual absolute refractory period.
The absolute and relative refractory periods are real phenomena. They are also observable phenomena: we can see that an atrial impulse arrived during the absolute refractory period of the AV node or His bundle because it failed to conduct in spite of more than adequate voltage. We can see that an atrial impulse arrived during the relative refractory period of the AV node or His bundle because it conducted with a prolonged PR interval. But observing these phenomena doesn’t really tell us exactly where the absolute refractory period ends and the relative refractory period begins.
The effective refractory period begins with a programmed stimulus (S1) and ends with a programmed stimulus (S2). S1 marks the beginning of Phase 0 of the action potential and S2 marks the longest interval from S1 that fails to result in a depolarization. Note that I did not restrict the longest interval to “within the absolute refractory period.”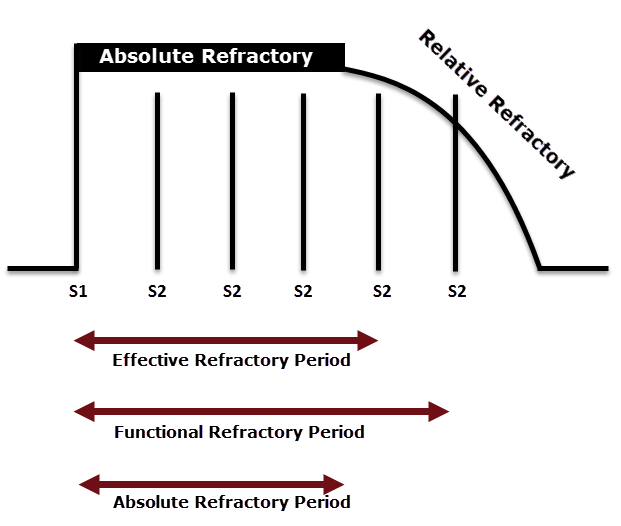
In the diagram above, there are 5 equal, vertical lines representing paced impulses (S2) following Phase 0 (S1) of the action potential. Only a line crossing through the curved line representing the relative refractory period has reached threshold and will result in an action potential. Here, only the 5th line breaches the relative refractory curve, so it conducted.
The length of the effective refractory period depends on the strength of the stimulus being used and the length of the coupling interval (number of msec between S1 and S2). If the stimulus is not very strong, the effective refractory period will be measured well into the actual relative refractory period before a depolarization appears (as in the diagram above). If a stronger stimulus is used, a depolarization will be produced earlier and the effective refractory period will be shorter and more representative of the absolute refractory period. Also, if the coupling interval is rather long, the last non-conducted S2 may occur well before the end of the absolute refractory period. So it’s possible that the effective refractory period may actually be measured as being longer or shorter than the absolute refractory period. Although the effective refractory period and the absolute refractory period are not always exactly equal, for practical purposes they can be considered almost the same (since the electrophysiologist’s attempts to measure the effective refractory period are obviously much more precise than depicted in the diagram above). The terms are frequently used interchangeably in the literature but now you understand the subtle difference.
Many people make the mistake of thinking that if the effective refractory period is “basically” the same as the absolute refractory period, then the functional refractory period is the same as the relative refractory period. Nothing could be further from the truth! The functional refractory period and the relative refractory period are not at all the same, though they both relate to the point during the action potential in which an extra-strong stimulus can result in a depolarization. The functional refractory period is the electrophysiologist’s attempt to measure the distance from the onset of the action potential to the onset of the relative refractory period – not the duration of the relative refractory period! It actually represents the shortest interval between two consecutively conducted, paced impulses (S1 and S2). The relative refractory period begins at the point during repolarization that an exceptionally strong stimulus can initiate a depolarization and it ends (usually, but not always) with the onset of Phase 4. This is not what the functional refractory period measures!
The electrophysiologist, however, finds it more practical to measure from a programmed stimulus (S1) that initiates an action potential to the earliest point at which a sufficiently strong stimulus (S2) is able to initiate another depolarization. Thus, the functional refractory period is a measurement between two programmed stimuli – once again, S1 and S2 – and covers all the same territory as the effective refractory period. But again, this determination is voltage- and time-dependent with the strength of the stimulus and the coupling interval (the interval between S1 and S2) affecting where the first depolarization occurs.
But note that while the effective refractory period and the absolute refractory period are virtually the same, the functional refractory period and the relative refractory period are measurements of different sections of the action potential. What we think of as the relative refractory period begins, basically, where the functional refractory period ends.
Note:
1. The effective refractory period is – by definition –shorter than the functional refractory period if the same stimulus strength and the same coupling intervals of S1 and S2 are used in both measurements.
2. The effective refractory period is (presumably) completely overlapped by the absolute refractory period while the functional refractory period and relative refractory periods overlap very little!
3. Both the effective refractory period and the functional refractory period begin and end with a programmed stimulus. The absolute refractory period and the relative refractory period are surmised based on the duration of the action potential (QT interval) and the response of the heart to the following sinus or ectopic impulse.
4. The effective refractory period essentially determines the end of the absolute refractory period while the functional refractory period determines the beginning of the relative refractory period.
The absolute refractory period ends around the time the membrane potential has returned to about -60°. Likewise, that is approximately where the relative refractory period begins.
Related Terms:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Clarification
I would like to clarify one of the statements in the monograph to be sure there is no misunderstanding. In discussing the determination of the effective refractory period, it states that the length of the ERP depends on the amplitude of the paced stimuli and the coupling interval (time between S1 and S2) used by the electrophysiologist to make the determination. More specifically (and correctly), it is not only the individual coupling intervals but the incremental increase in the coupling intervals, i.e., the amount by which each coupling interval is increased.
For instance, if the electrophysiologist was using a stimulus with a near-maximal amplitude and was increasing the coupling interval by 20 msec each time, a pulse that fell 1 msec outside the end of the absolute refractory period would conduct and thus the end of the effective refractory period would actually be measured about 19 msec before the end of the actual absolute refractory period. However, using the same pulse amplitude, if the coupling intervals were being increased by only 5 msec each time and the near-maximal stimulus fell 1 msec beyond the end of the absolute refractory period and conducted, the end of the effective refractory period would be measured just 4 msec before the end of the absolute refractory period and the effective refractory period would better approximate the absolute refractory period.
Jerry W. Jones MD FACEP FAAEM
https://www.medicusofhouston.com
Twitter: @jwjmd