
Submitted by Dawn on Sat, 06/22/2013 - 22:01
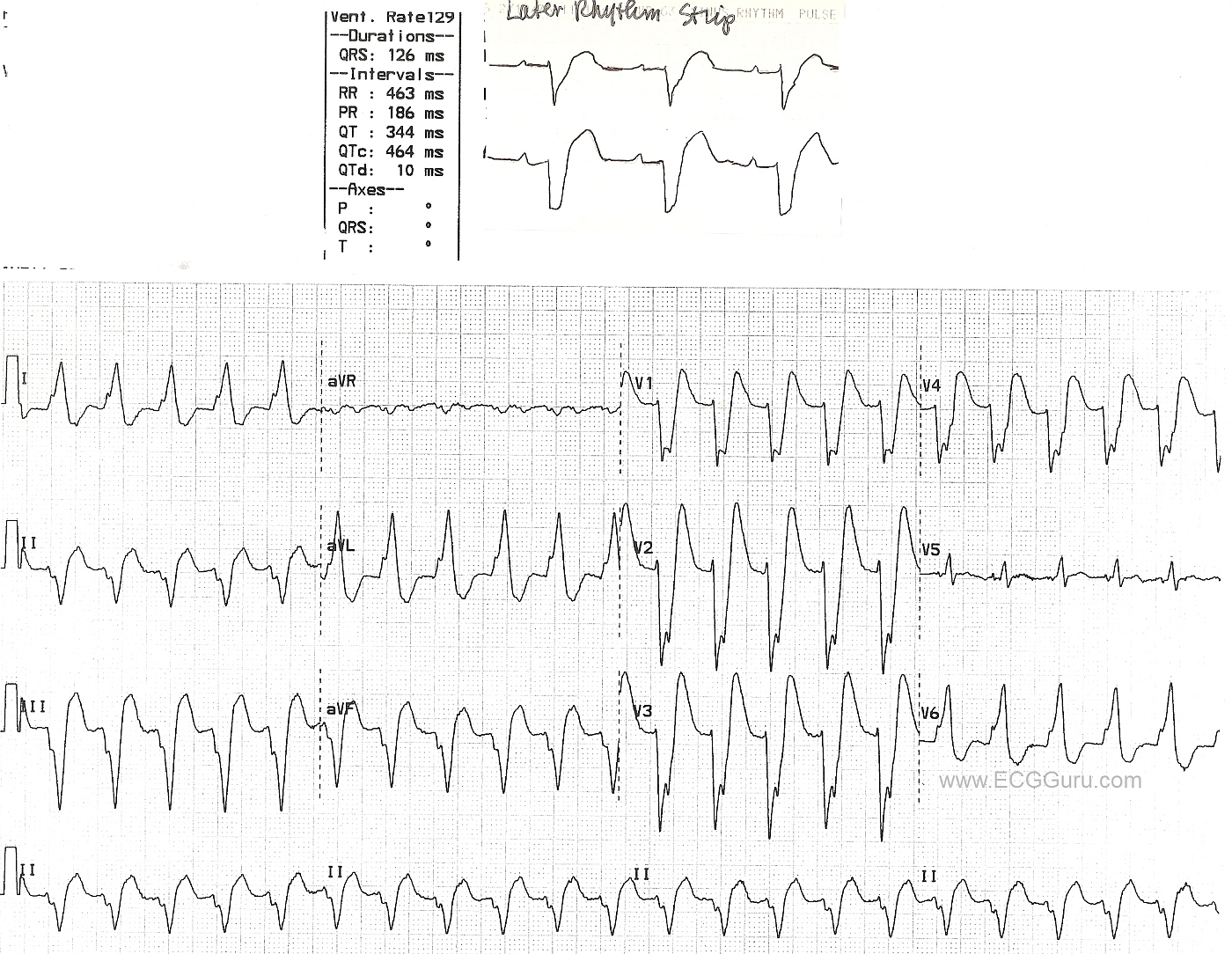
This wide complex tachycardia has an initial rate of 129/min. It is difficult to discern if P waves are present, although the ECG machine does give us a PR interval. The ECG meets most of the criteria for left bundle branch block: wide QRS, negative QRS in V1, positive QRS in Lead I and V6.The axis is leftward, which is common in LBBB. However, it is difficult to say for certain that this is a supraventricular rhythm. Later, however, the patient's rate slowed (see top strip), revealing P waves. When the rate slowed, the left bundle branch block pattern remained. That helps confirm the original interpretation of left bundle branch block. Interestingly, the BBB is not rate-related, in that it is still present at the slower rate.
Of course, it would be helpful to have a complete 12-Lead ECG after the rate slowed, and it would also be good to see the onset and/or offset of the fast rhythm, which would help to determine if this is a sinus tachycardia or a paroxysmal supraventricular tachycardia (PSVT). We do not have clinical data to help us determine if a sinus tachycardia with a rate of around 130 / min. would be appropriate or expected in this patient.
Click on image, or, for best image quality, right click and SAVE image.
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Regular WCT Rhythms are Not Always VT ...
I looked at the 12-lead ECG first. I see a regular WCT (Wide-Complex Tachycardia) at ~135/minute without clear sign of atrial activity (despite what the computer says about the "PR interval" - ). The differential diagnosis for this is:
Statistically - the odds of a regular WCT without P waves being VT are at least 80% before you look at the tracing (confirmed by studies in the literature). This goes up to >90% if the patient is older and has underlying heart disease - which is why the diagnosis should always be thought of as, "VT until proven otherwise; Treat accordingly." That said, >90% is not 100% .... - and the follow-up rhythm strip shown here proves this to be one of the <10% of regular WCTs that turned out to be supraventricular.
For anyone with interest in Review of ECG Criteria for distinguishing between VT vs SVT (and how to treat when you are uncertain) - GO TO: https://www.kg-ekgpress.com/acls_comments-_issue_11/ -
Ken Grauer, MD www.kg-ekgpress.com [email protected]
P wave
Do I see P wave v5?? Review od V5 these are waves of QRS as compared to v4
opinion
There is a saying if LBBB AND LOOKS like LBBB then it is unlikely to be VT; atypical LBB are worrisome. secondly we dont see Q in V6.
KEN can you please by your huge experience and knowledge share how LBBB LOOKS help in clinching ischemic versus non ischemic kind thanks
aaa
REPLY to Opinion
Ken Grauer, MD www.kg-ekgpress.com [email protected]