
Submitted by Dawn on Wed, 03/16/2016 - 22:55
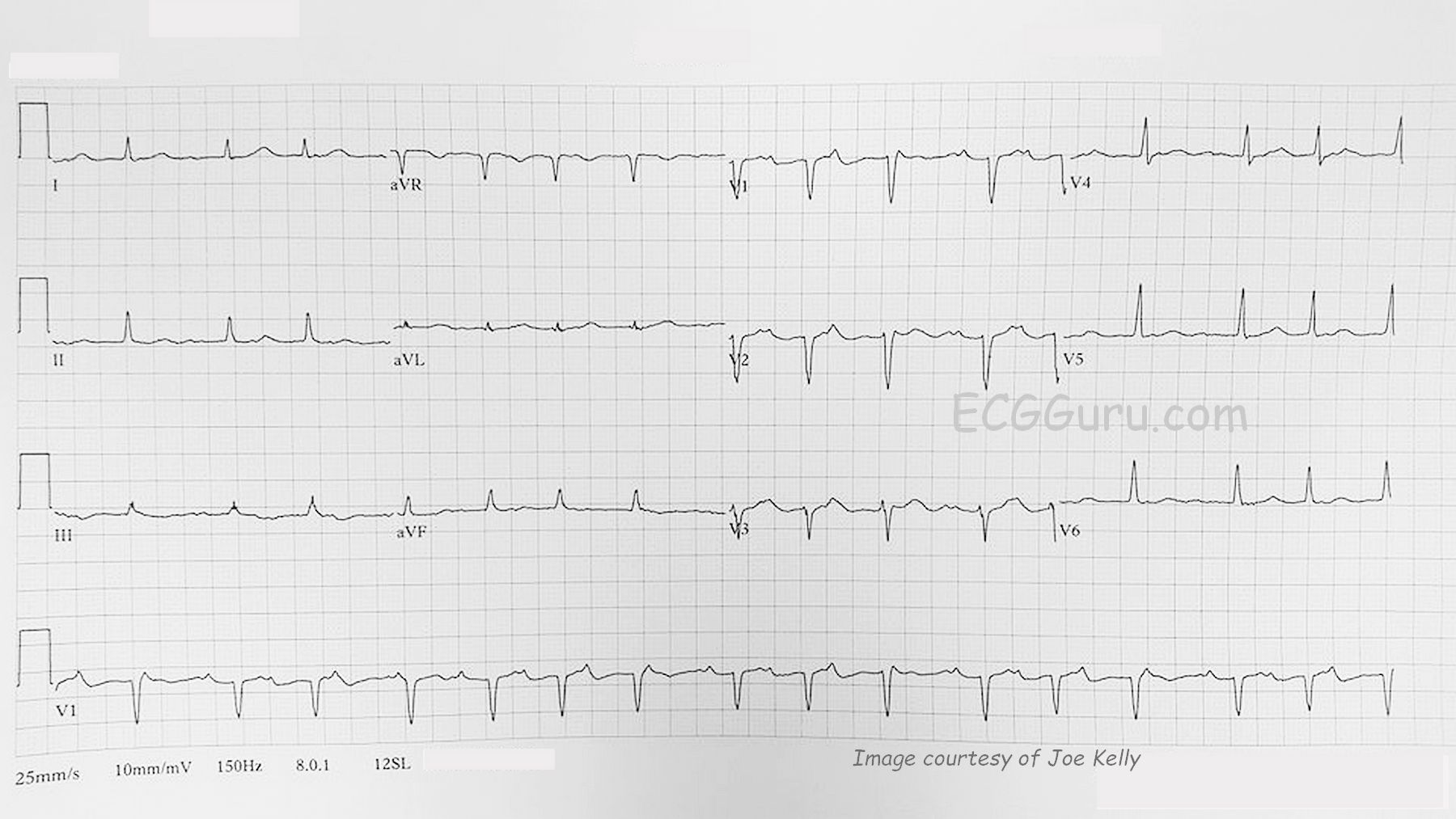
This ECG was obtained from a patient in a walk-in health clinic. We do not have any other information on the patient. We thank Joe Kelly for donating this interesting ECG to the GURU.
IRREGULAR RHYTHM If you march out the P waves, you will see that they are regular, at a rate of approximately 130 bpm. But the QRS complexes are not regular, and there are fewer QRS complexes than P waves.
WENCKEBACH CONDUCTION Looking closely at the PR intervals, you will notice that they progressively prolong. This “pushes” the QRS complexes progressively toward the right. Eventually, the T wave – and the refractory period – will land on the next P wave. That P wave will be unable to conduct to the wave, and no T wave of course, so the next P wave will conduct with a shorter PR interval.
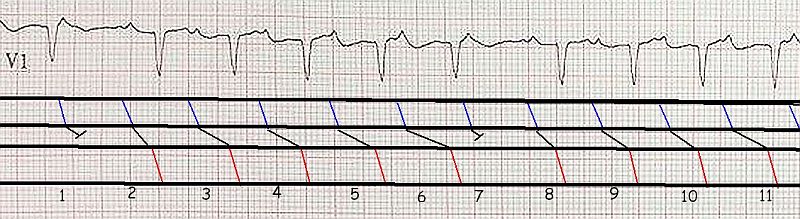
We are including a short rhythm strip from this patient, with conduction marked with a laddergram.
NOT A TYPICAL PRESENTATION If your students have always learned “Second-degree AV block, Type I” or “Wenckebach” on a rhythm generator, they will expect to see a normal sinus rhythm, not sinus or atrial tach. They will also expect to see clearly repeating cycles of progressively prolonging PR intervals, until one P wave is non-conducted, producing a slight pause. They may not recognize the cause of the irregularity in this ECG unless they systematically analyze the P wave rhythm and then the QRS complexes and PR intervals. In this patient, V1 probably has the clearest P waves for analysis, and there is a continuous V1 rhythm strip on the bottom of the page.
For those more advanced students, there are some “atypical” aspects to this ECG. You may notice that the FIRST P-QRST in each cycle has a PR interval of about .22 seconds, EXCEPT for the fourth beat on the 12-Lead ECG. This one appears to have a very SHORT PRI, but it is more likely that the PR interval was so LONG, the QRS appeared slightly AFTER the next P wave. What do you think?
BOTTOM LINE We are hoping some of our experts, including our Consulting Expert, Dr. Grauer, will add more detailed comments to this ECG. The main points we would like to make on the most basic level are:
1) Real ECG rhythms may vary quite a bit from the basic examples seen on electronic rhythm generators, and in some brief references.
2) The “AV block” in this case is not a worrisome condition – it is more an expected lack of conduction due to a P wave landing in a refractory period. This is called “physiological block”. I would be more concerned about why this patient has tachycardia, and the clinical approach would be to evaluate the patient’s heart rate in light of his or her presenting symptoms.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
dual AV nodal pathways?
An interesting ECG from Dawn and, as she suggests, not completely straightforward. The first thing I would question is the underlying rhythm. It may well be sinus tachycardia at 130 bpm, but the P waves in the limb leads, particularly lead II, would normally be much more prominent if that were the case, and my understanding is that sinus tachycardia is not commonly associated with Wenckebach block. My guess is that this is an atrial tachycardia, but I can’t be sure. The other interesting thing, as pointed out by Dawn, is the short PR interval of the 4th QRS in the 12-lead. A short PR interval of the beat after the blocked P wave is quite commonly seen in Wenckebach block , due to the occurrence of a junctional escape beat terminating the pause, in which case the P wave after the pause is not conducted and the PR interval is therefore not a ‘genuine’ one. In this case, however, the first QRS after the pause is unlikely to be a junctional escape because it comes in after an RR interval of only 720 ms. I think, therefore, that the QRS after the pause is likely to be a conducted beat and linked to the P wave on the T wave of the previous beat. If this is true, then there is a big jump in PR interval from the 3rd to the 4th beat, and this perhaps suggests the presence of dual AV nodal pathways with a switch in conduction from the fast to the slow pathway on beat 4.
Dave R
Mobitz I plus Dual AV Nodal Pathways
Our thanks to Joe Kelly for submitting this interesting case to the ECG Guru. GREAT comments by David Richley, that I completely agree with. The atrial rhythm is almost (but not completely) regular at ~ 130/minute. But given the lack of a clearly upright P wave in lead II on the 12-lead ECG in the face of somewhat unusual P wave morphology in lead V1 (pointed P wave much larger than size of the P in lead II) — this is almost certainly atrial tachycardia (ATach). ATach may be somewhat irregular — and measurement of the P-P interval here across the rhythm strip is indeed more irregular than sinus tachycardia usually is at this rate.
As per Dawn — not all of our patients “read the textbooks” — and this example of Wenckebach conduction is clearly not typical. Nevertheless, the clues are there — as we see “group beating” — a fairly regular atrial rate — and PR interval lengthening until a beat is dropped, after which a similar (although not quite the same) cycle resumes. A BIG clue to me that this is Wenckebach comes with recognition that the 1st beat at the end of the relative pause (ie, beats #2 and #8 in the laddergram) end the relative pause with the same PR interval — which unequivocally tells us that these beats are conducted! Once we recognize beats #2 and 8 are conducted — it becomes far easier to see that subsequent P waves are also conducted, albeit with different (and increasing) PR intervals, until a beat is dropped.
But as David Richley astutely points out — this is not a “typical” Wenckebach periodicity. That’s because the R-R interval within groups of beats does not gradually and progressively decrease until the pause. With typical Wenckebach periodicity in 2nd-degree Mobitz Type I AV block — the greatest “increment” in PR interval is most often between the 1st and 2nd beats in any cycle. That clearly is not what is happening here — in which unpredictable jumps in the PR increment are seen at various points in the tracing. This unpredictable change in PR interval from one-beat-to-the-next suggests that in addition to AV Wenckebach, dual AV Nodal pathways are operative, with the unusual change in PR interval increment being due to alternation between one and the other AV nodal pathway which each conduct at different velocity.
BOTTOM LINE: There are several important teaching points to take away from this highly interesting rhythm strip. The atrial rate is too fast — so clinically we need to determine why. The rhythm is probably not sinus tachycardia, given abnormal P wave morphology — but rather atrial tachycardia. In days gone past, (when use of Digoxin was far more common) — the most common reason for ATach with AV Block used to be Digoxin toxicity, so inquiry should be made as to whether this patient was taking Digoxin (or other cardioactive medication). Identifying P waves, group beating, and clear evidence that the beat ending each relative pause (in the long lead V1 under the 12-lead tracing) seems to be conducted with the same PR interval should suggest Wenckebach-like conduction — with unpredictable variation in PR interval increment from one-beat-to-the-next suggesting that this example of Mobitz I is associated with dual AV nodal pathways.
===================
Additional Reading — For more on the concept of Dual AV Nodal Pathways — CLICK HERE —
Ken Grauer, MD www.kg-ekgpress.com [email protected]
Thanks, Dave and Ken
I was hoping you would address the strange PRI progression, and you have explained it so well. You also caused me to take a second look at P wave morphology, and agree with you both that these P waves look ectopic. So, atrial tach seems the much more likely diagnosis. I am editing the title of this ECG to make it more accurate for those searching the content of the ECG Guru. Thanks again to both of you!
Dawn Altman, Admin