
Submitted by Dawn on Thu, 12/04/2014 - 23:47
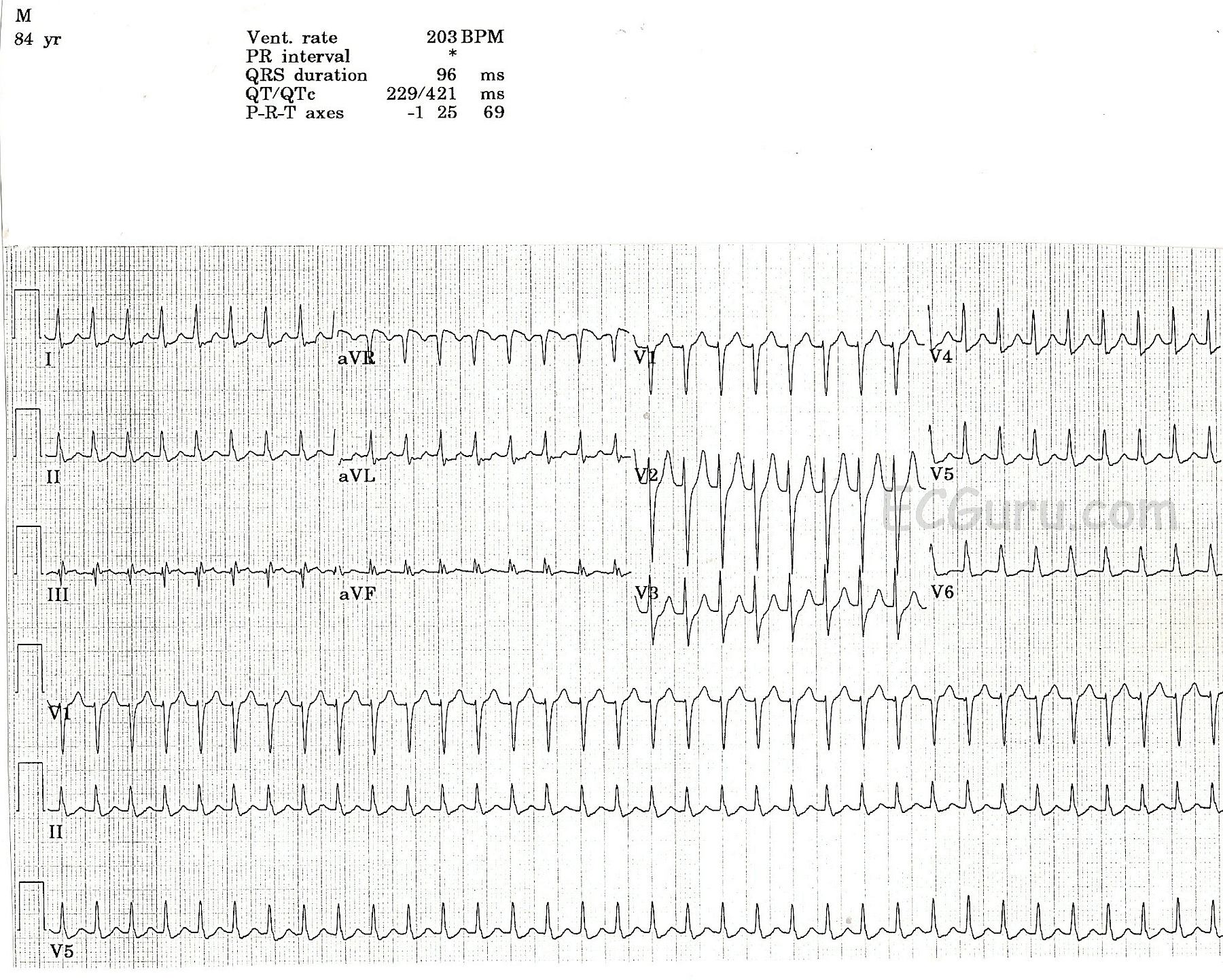
This ECG shows AV nodal reentrant tachycardia in an elderly man. Clinical information is not available. AVNRT is the rhythm most often associated with the term, "supraventricular tachycardia".
Although we can't see the beginning of this rhythm, one of the identifying features of SVT is an abrupt (paroxysmal) onset. In patients with AVNRT, there are two pathways in the AV node, a pathway with fast conduction and a long refractory period, and a pathway with slow conduction and a short refractory period. Normal sinus impulses travel down the fast pathway and into the ventricles, but also start up the slow pathway in a retrograde direction. The retrograde impulse and the normal impulse traveling down the slow pathway collide, cancelling each other out. If a PAC occurs, it will travel down the slow pathway while the fast pathway is still refractory. By the time the impulse reaches the end of the slow pathway, it finds the fast pathway no longer refractory, and travels back up to the atria. This forms a circular movement (circus movement) of the impulse, and it repeats itself rapidly until interrupted. When each impulse reaches the ventricles, it travels into the interventricular conduction system and causes ventricular depolarization and contraction, usually at a rate of 140 - 250+. Unlike sinus tachycardia, AVNRT does not adjust its rate according to the needs or activity of the patient.
There are many forms of supraventricular tachycardia, and they are not always easy to differentiate based on ECG criteria alone. AVNRT of the type described above is the most common PSVT in structurally normal hearts. For more information on supraventricular tachycardia, go to Life in the Fast Lane. For a discussion on clinical management, we recommend Dr. Grauer's ECG Video 6 - Rhythm Mgmt-Part 3.
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
AVNRT on a 12-lead
Ken Grauer, MD www.kg-ekgpress.com [email protected]