
Submitted by Dawn on Thu, 08/06/2015 - 20:56
We originally published this ECG in 2012. It was generously donated to the ECG Guru website by our friend and ECG Guru Extraordinaire, Jason Roediger. We are re-publishing it today, as it is a great ECG for illustrating how helpful laddergrams can be for showing conduction in dysrhythmias.
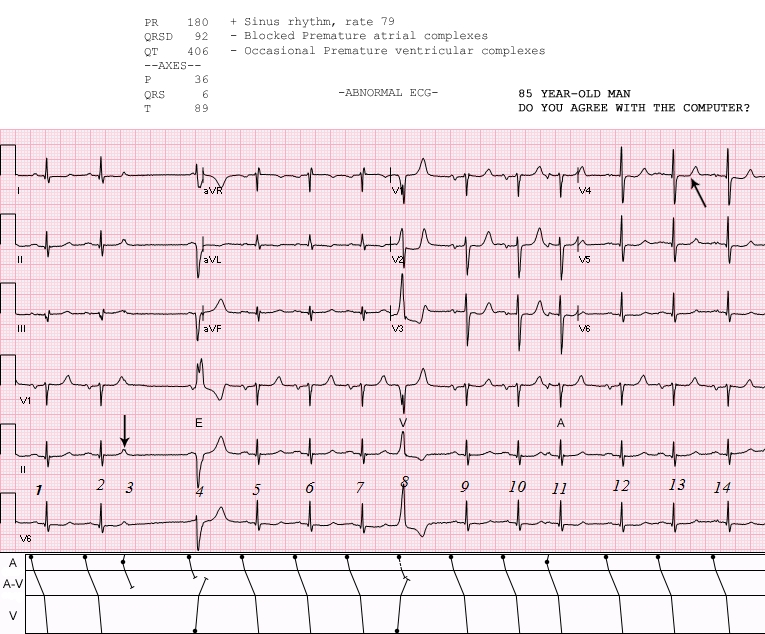
This ECG has something for everyone: The rhythm is sinus, and there is a non-conducted PAC (beat number 3) after the second beat. Just after the next P wave, there is a ventricular escape beat which prevents that P wave from making a QRS. The eighth beat is a PVC. The eleventh is a conducted PAC. You can use this ECG to illustrate for your students the concepts of "escape" beats, refractory periods, and premature beats.
There are ST changes that suggest coronary artery disease: the ST segments are flat in shape with a tiny amount of elevation in V1 through V4. The axis is normal, at the border of normal and left axis. It is difficult to see, but there appears to be a tiny r wave in Lead III, so we cannot say for sure if there is or was a pathological Q wave in that lead.
The P waves are wide and "double" in Lead II and biphasic in V1, suggesting LV failure or mitral valve disease. However, the criteria for LV hypertrophy are not met.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
LADDERGRAM Review of Basic Arrhythmia Elements
Ken Grauer, MD www.kg-ekgpress.com [email protected]