
Submitted by Dawn on Thu, 03/20/2014 - 10:31
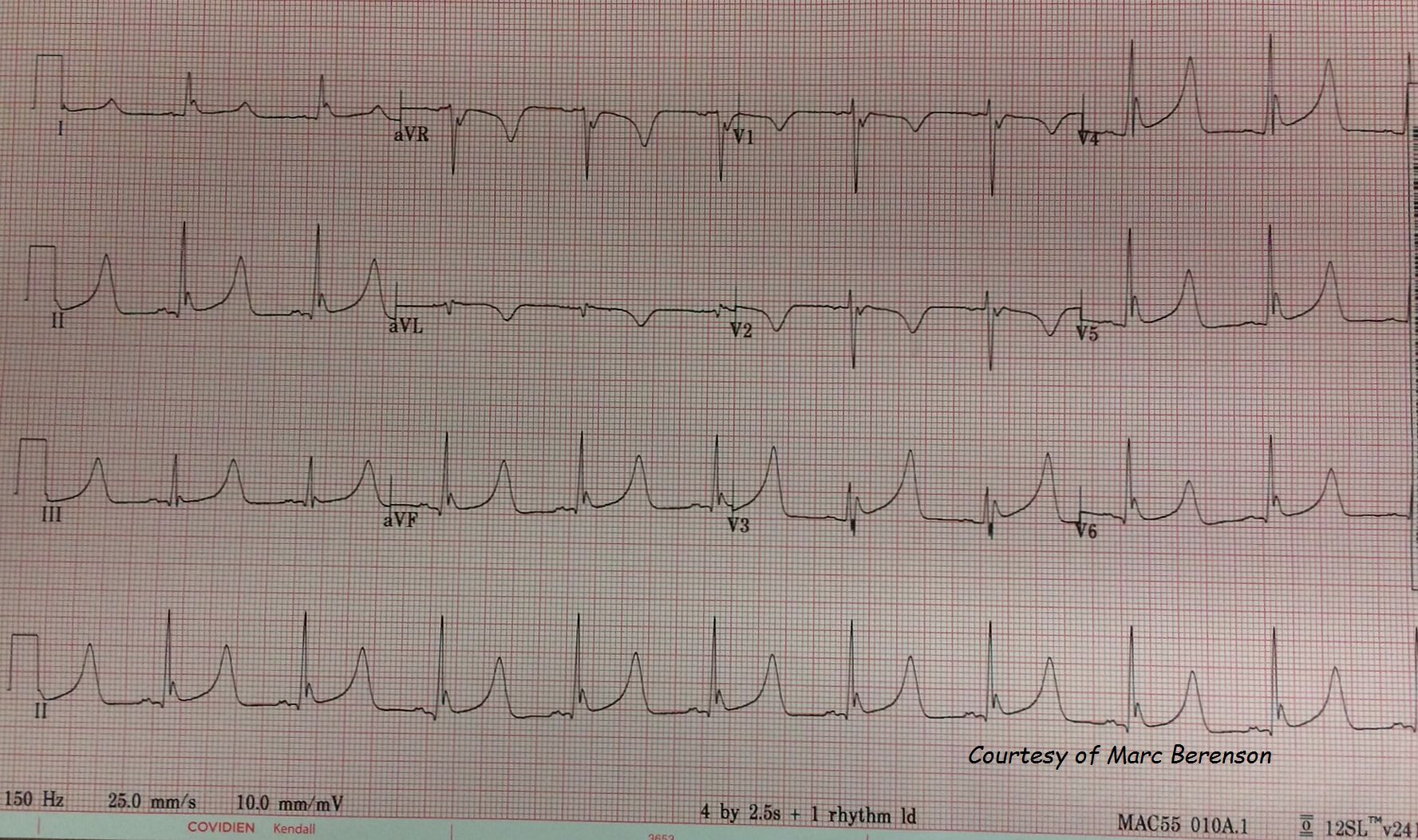
This is one of the best depictions of Osborn waves you will find. It was first published on FaceBook, on the EKG Club group. The owner of this tracing, Marc Berenson, has graciously allowed us to publish it here for the use of our members.
This ECG is from an unresponsive patient with a Glasgow Coma Scale of 3. His core temperature was 86 degrees F (30 degrees C). He was not moving or shivering. He was found to have a brain mass with bleeding, causing herniation of the brain stem.
Osborn waves are caused by hypothermia, and also by a number of other conditions. They are best described as an “extra” wave at the J point (junction of the QRS complex and ST segment). They are sometimes called “camel hump waves”. Hypothermia can also cause many other cardiac problems, including prolongation of the PR interval and QT interval, arrhythmias, and eventually asystole.
In this case, the hypothermia was probably caused or exacerbated by the patient’s loss of thermoregulation due to the brain bleed. Neurological insults such as subarachnoid hemorrhage, and head trauma can cause Osborn waves, and this patient certainly was in that category, along with being demonstrably hypothermic. Other causes of Osborn waves include hypercalcemia, some medications, and as a normal variant.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Osborn Waves vs Early Repolarization
Ken Grauer, MD www.kg-ekgpress.com [email protected]