
Submitted by Dawn on Tue, 10/26/2021 - 14:20
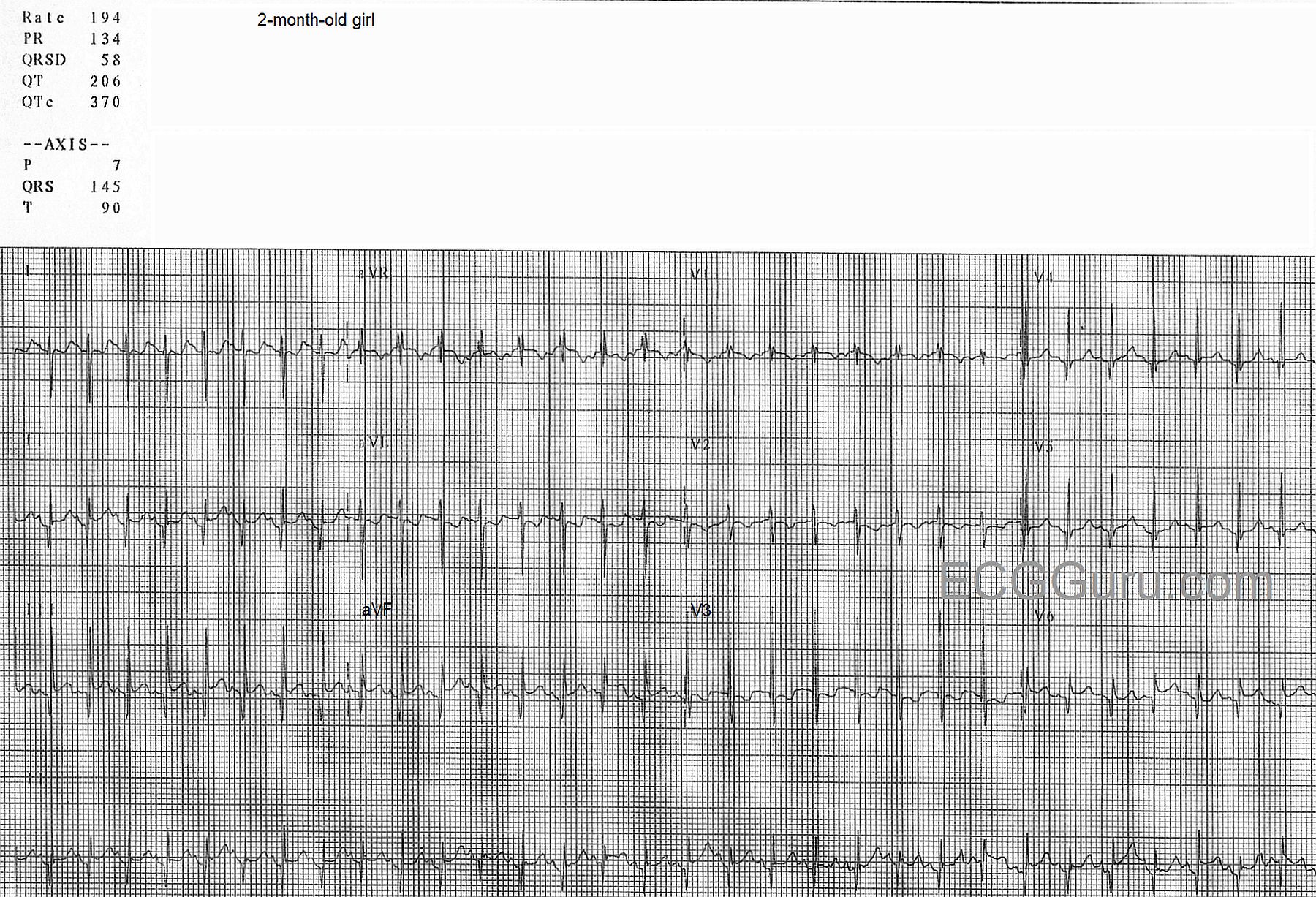
The patient: This ECG was obtained from a two-month-old girl who was a patient in the Emergency Department. She had a fever due to a respiratory infection and was dehydrated. She was alert, active, and irritable.
The ECG: There is a narrow-complex tachycardia at a rate of 194 bpm. This is faster than the normal range for a two-month-old, which is about 80-160 bpm. The intervals are all within normal range. The frontal plane axis, at 145 degrees, is rightward, which is normal for this age. There are prominent, narrow Q waves in the inferior wall leads (II, III, and aVF) and in the left lateral leads (V4, V5, and V6). There are no Q waves in the high lateral leads (I and aVL). This is a normal pattern for this age group. www.sciencedirect.com/science/article/pii/B9781416037743100280
The evaluation of this ECG must be preceded by a thorough evaluation of the patient. SINUS TACHYCARDIA would be expected in the setting of fever, dehydration, hypoxia, pain or other discomfort. Should the rate fail to gradually return to a normal range after treatment, we would have to consider a reentrant supraventricular tachycardia. Reentrant tachycardias have a SUDDEN ONSET and SUDDEN TERMINATION.
Unfortunately, we do not have follow up on the patient.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Sinus Tach at 200/Minute in a 2-Month Old
Most adult providers have limited exposure and limited experience interpreting pediatric ECGs. As a result — interpreting the ECG of an acutely ill child is often extremely challenging (if not downright intimidating). All of the "normals" that our years of experience with adult electrocardiography have taught us do not apply — as criteria for rate, axis, chamber enlargement, conduction defects and ischemia are all very different. And, many of the arrhythmias encountered with acutely ill children are just not the same as those we are used to looking for with adults.
That said — the basic systematic approach for interpreting an ECG is the same. Dawn has gone through these standard parameters for today's tracing:
— The marked right axis is not necessarily abnormal.
— The incomplete RBBB is to be expected.
— The Q waves in multiple leads is probably of no concern.
To this I would add 2 Points:
I calculate the heart rate here at slightly more than 200/minute. I bring this up not to "nit-pick" — because the clinical difference between a heart rate of 194/minute vs 200-205/minute is "nil". My reason for bringing up heart rate is because it will often be important to rapidly and very accurately calculate heart rate.
— Use of the "Every-Other-Beat" Method (described by me in detail in ECG Blog #210) facilitates this. When the heart rate is rapid and regular — simply pick a QRS complex that begins on a heavy grid line (1st RED line in my Figure-1 below).
— Note that 2 beats (RED numbers) occur in a little bit less than 3 large boxes (BLACK numbers). This means that HALF the rate = a little bit more than 300 ÷3 = 100/minute.
— Therefore, the actual rate = 200-205/minute (See the Video in Blog #210).
As to the rhythm — RED arrows appear to point to sinus P waves (upright in lead II). I see no evidence of any "extra" P waves from 2:1 AV conduction. Therefore, the rhythm is sinus tachycardia at ~200-205/minute.
— In adults — it is rare for sinus tachycardia to exceed 160-170/minute in a hospitalized patient (ie, in someone who has not just been running or exercising). But — All bets are off in pediatrics! This is because it is not uncommon to see sinus tachycardia at rates that exceed 200/minute, especially in infants who are acutely ill from dehydration. Chances are for the 2-month old patient in today's case, that the heart rate will rapidly decrease with fluid resuscitation (and THEN it will be important to precisely estimate heart rate — so that you can know that your treatment is moving in the right direction!).
For More on the Above Concepts, Please SEE:
— ECG Blog #210 — Reviews the "Every-Other-Beat" Method for rapid and accurate rate estimation when the rhythm is very fast (Please see the 3-minute ECG Video in this blog post for review of my method).
— ECG Blog #122 — Reviews in detail the interpretation of a pediatric ECG case (Please check out the links I provide in the Additional Reading section at the bottom of this blog post for more on the Basics for Interpretation of Pediatric ECGs).
Ken Grauer, MD www.kg-ekgpress.com [email protected]