
Submitted by Dawn on Thu, 08/07/2014 - 21:57
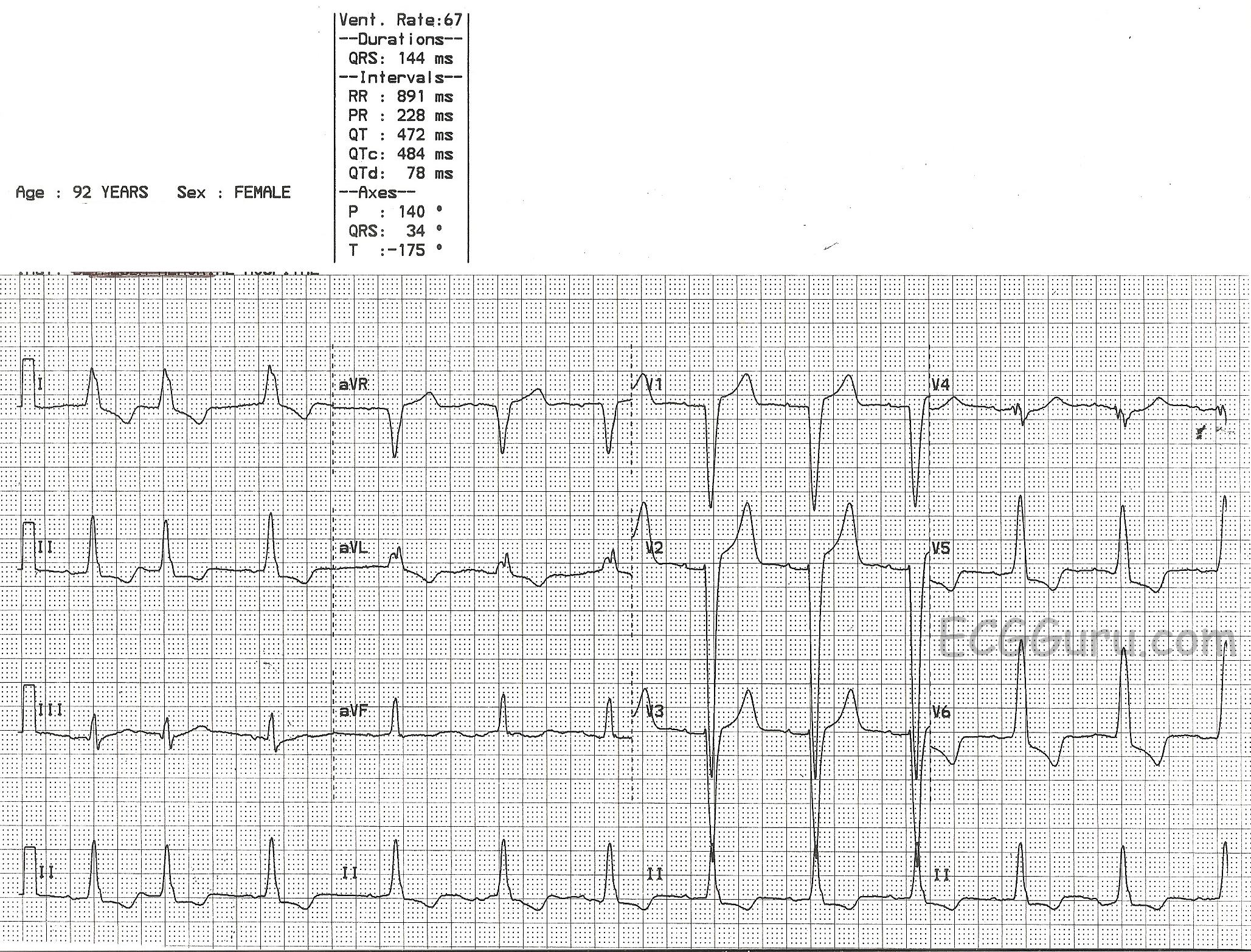

This is a good example of sinus rhythm with left bundle branch block. There is some irregularity due to a PAC at the beginning. The QRS is wide at 144 ms (.14 seconds). There is also first-degree AV block, with a prolonged PR interval of 228 ms. The criteria for diagnosis of left BBB are: wide QRS, supraventricular rhythm, and a negatively-deflected QRS in V1 with a positive QRS in Leads I and V6.
Left bundle branch block can be associated with many forms of heart disease, including CHF. It can be permanent, transient, intermittent, or rate-related. The wide QRS of LBBB significantly decreases cardiac output, causing poor perfusion symptoms in some people.
This ECG is a good one for your students who are just transitioning from reading rhythm strips to reading 12-lead ECGs. It shows the value of multi-lead assessment of rhythms. You will notice that P waves are difficult to see in some leads. Armed with the knowledge that the four channels on this ECG are run simultaneously, you can show the students how finding P waves in one lead will allow you to find them in the leads that are above and below that lead.
Similarly, it can be difficult to see the QRS width in some leads. The leads in the same vertical column can help you see the QRS's true width, even if part of the QRS is "flat" in the isoelectric baseline.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Features of Complete LBBB
Ken Grauer, MD www.kg-ekgpress.com [email protected]