
Submitted by Dawn on Tue, 10/15/2013 - 01:02
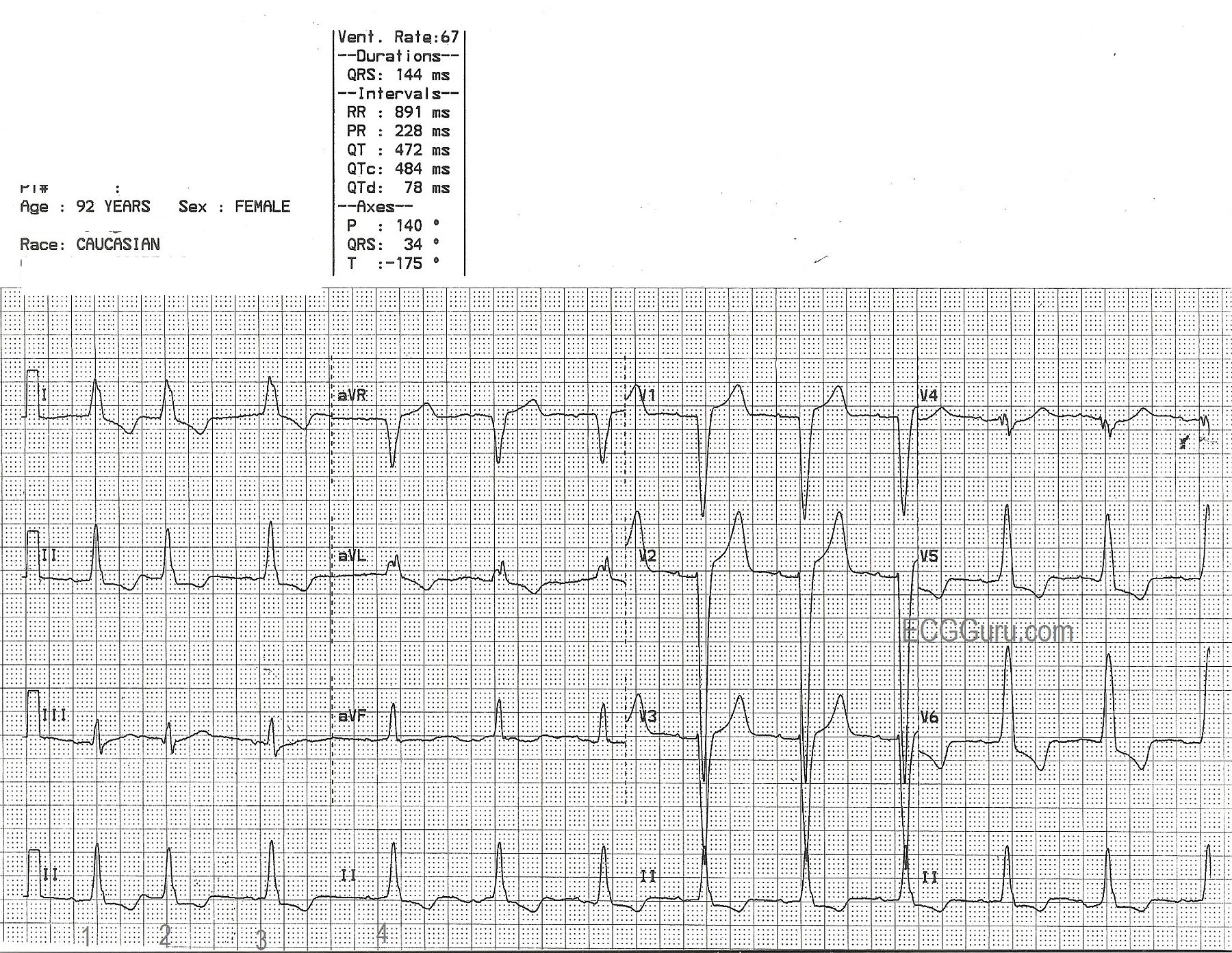
This ECG offers a good example of the left bundle branch block pattern. * The QRS is wide at 144 ms. * There is a supraventricular rhythm - in this case, normal sinus rhythm with beat number two a PAC, and a slightly prolonged PR interval. * The QRS is negative in V1 and positive in V6 and also Lead I. This satisfies the ECG criteria for left bundle branch block.
The main lesson this tracing offers for beginner or refresher students is the value of multi-lead assessment. Using only one or two leads, you may miss important information needed to correctly interpret the ECG. In order to meet the LBBB criteria, we must show that there exists a supraventricular rhythm (not ventricular). One easy way to prove the rhythm is supraventricular is the presence of P waves. In this ECG, P waves are very small, and are invisible in some leads, such as Lead I, aVL, Lead III, and aVF. P waves can be seen well in Lead II and in the chest leads. Some helpful hints, if viewing on a computer, enlarge the image to better see the P waves. Look at the ECG machine's interpretation. If a numerical PR interval is given, and a P wave axis, then the computer is finding P waves. If you don't see them in one lead, try others.
For your more advanced students, ST elevation is common in wide-QRS rhythms, occuring in leads that have a negative QRS complex. Conversely, ST depression will be seen in leads with wide, upright QRS complexes. This makes the ECG with LBBB very confusing to read. Evaluation of the ST segments should be deferred to experts. Most EMS field protocols allow for a STEMI Alert to be called in LBBB only if the LBBB is known to be new-onset and the patient has obvious cardiac symptoms. You can find many more examples of LBBB on this site, even LBBB with acute MI.
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
12 Leads are Better than One
Ken Grauer, MD www.kg-ekgpress.com [email protected]