
Submitted by Dawn on Wed, 09/26/2012 - 16:04
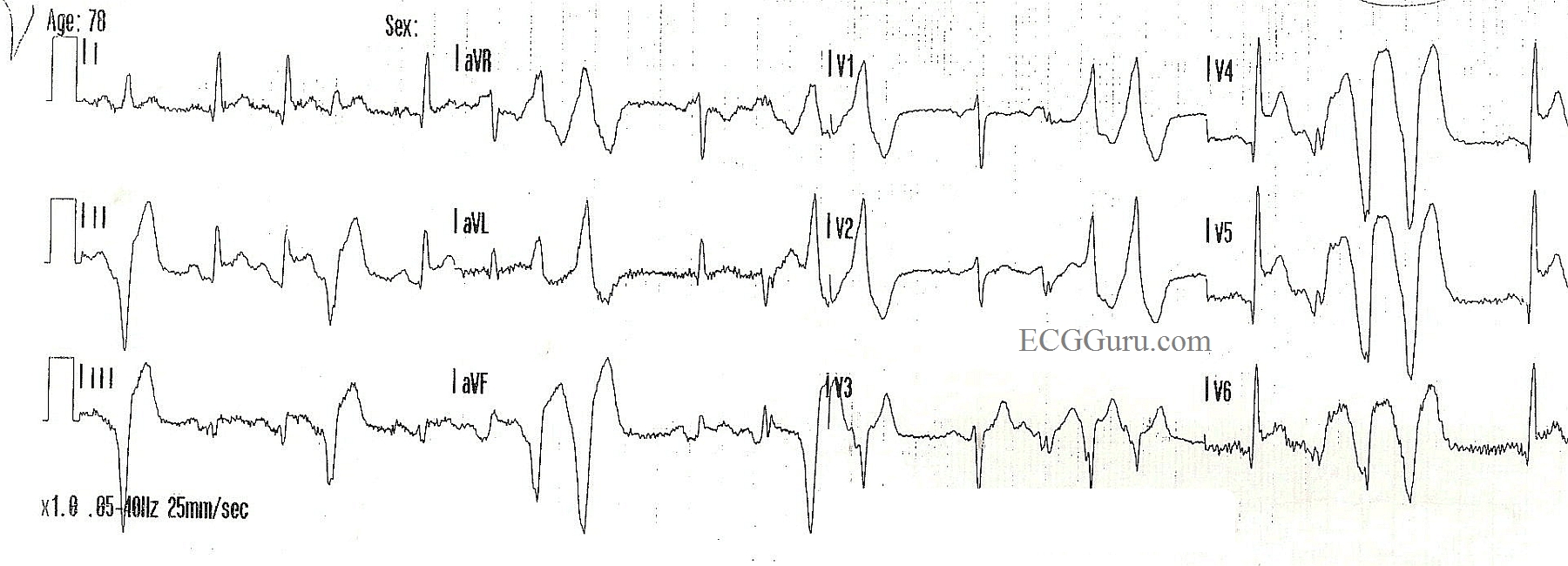
Unbelievably, this inferolateral ST elevation M.I. was missed by the treating paramedics in the field. An elderly woman stepped off a curb and was hit by a very slow-moving car. She fell and sustained a Colle's fracture of the right wrist. While the paramedics assessed her, she complained of chest pain, prompting them to perform a 12-Lead ECG. The machine's interpretation called attention to the inferior and lateral walls' injury pattern, but the paramedics did not believe it, because "she was a trauma patient". They ran three ECGs, and still did not agree with the machine.
The patient was transported to a hospital without an interventional cath lab, and she was forced to endure a one-hour wait to be transferred to an appropriate hospital.
This is a great ECG for a discussion with your students about "distractors". The call came in as a trauma, so that, in itself, was a distractor. The rescuers saw what they expected to see. The angulated fracture distracted them - putting them into full trauma assessment mode. Then, the frequent and coupled PVCs also distracted them, possibly making it more difficult for them to evaluate the ST segments in the normal beats. Interestingly, the second and third ECGs did not have PVCs, and the ST elevation was even more clear.
PVCs which are repeating themselves in groups of two, three, or more are sinister in a chest pain patient, and may indicate LV dysfunction. They could possibly result in ventricular tachycardia, which would be disasterous for this patient.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Distractors
It is unfortunate but we have all "tunneled" in on calls seeing one thing that just shuts off our brain to the real problem before us. We recently flew a pt out of a trauma center to a stroke center, pt was an elderly woman MVC, but had a stroke prior to the MVC with very clear signs, droop drift and slurring, no trauma, minor MVC .
Bill Rice, RN,CEN,CFRN
Distractors - shouldn't distract from Systematic Approach
The BEST learning often comes from the most 'painful' cases - this one being an excellent example of what I'm sure in retrospect seems perfectly obvious - but wasn't in the midst of a challenging call in a patient with trauma who 'wasn't supposed to be having an acute MI' ....
That said - one of the LESSONS to be learned is to ALWAYS be systematic in one's interpretation of 12-leads. One must assess 6 parameters on each 12-lead tracing = Rate - Rhythm - Intervals (PR/QRS/QT) - Axis - Hypertrophy (chamber enlargment) - and Changes of Infarct (= looking at ALL 12 leads for the presence of Q waves - R wave progression and ST and T wave changes). Had one done so - then the Q waves and ST elevation in infero-lateral leads would have been seen.
Ken Grauer, MD www.kg-ekgpress.com [email protected]