
Submitted by Dawn on Tue, 02/14/2012 - 21:39
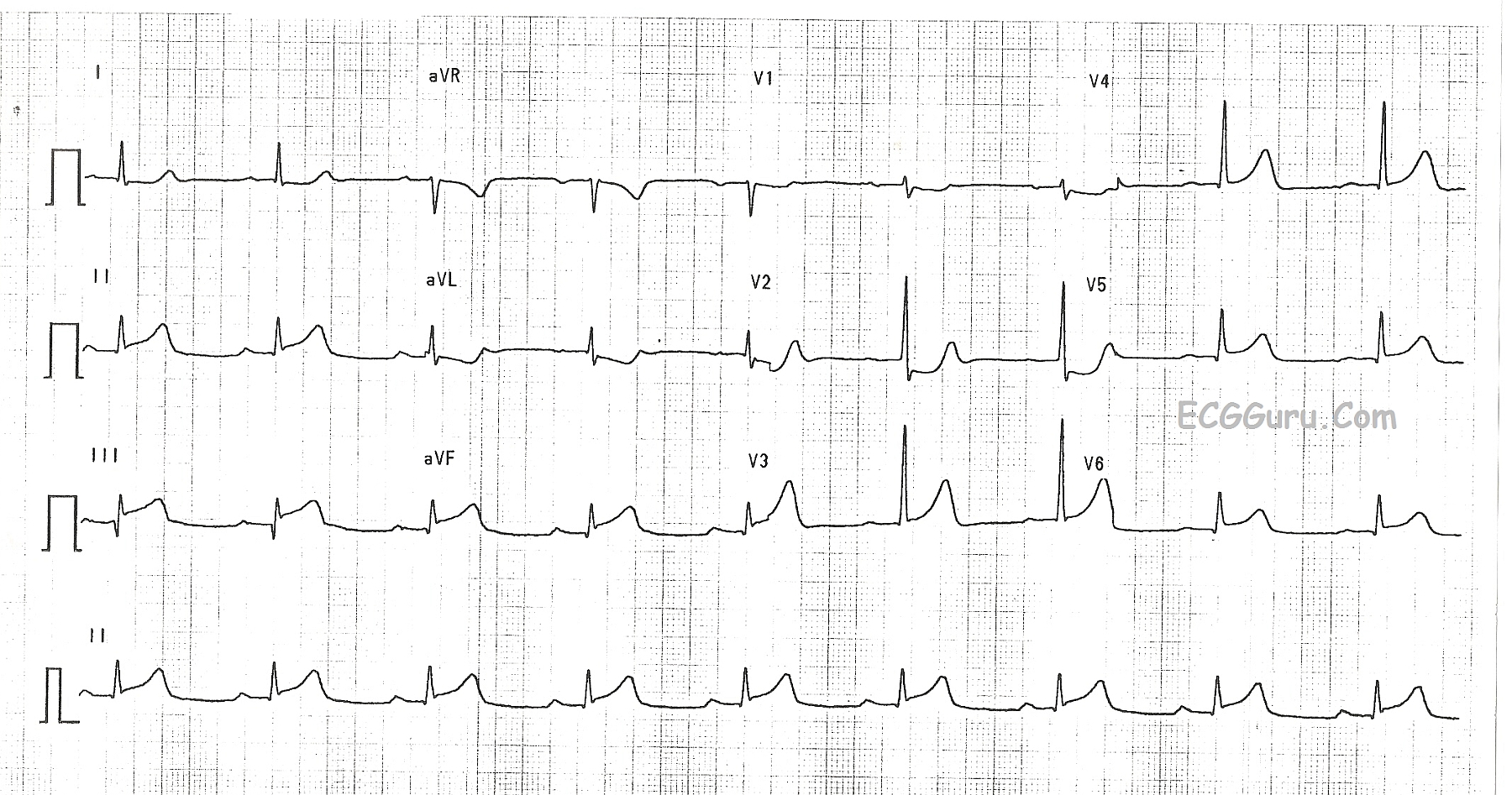
This ECG shows a classic inferior - posterior STEMI. This M.I. was due to complete occlusion of the right coronary artery. ST elevation apparent in Leads II, III, and aVF show the acute injury in the inferior wall, while ST depressions in V1 and V2 are reciprocal of the ST elevations in the posterior wall. The tall R waves in Leads V1 - V3 most likely are reciprocal to pathological Q waves in the posterior wall. Tall R waves in the right precordial leads can be caused by other cardiac conditions, such as right ventricular enlargement. RV hypertrophy can probably be ruled out in this case because there is no right axis deviation or P pulmonale. Because inferior wall M.I.s often extend into the posterior wall, it is the most likely cause of the tall R waves.
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Infero-Postero MI: acute RCA vs dominant LCx occlusion?
Excellent illustrative example by Dawn of acute infero-postero MI. I'd add the following points to her explanation:
Ken Grauer, MD www.kg-ekgpress.com [email protected]