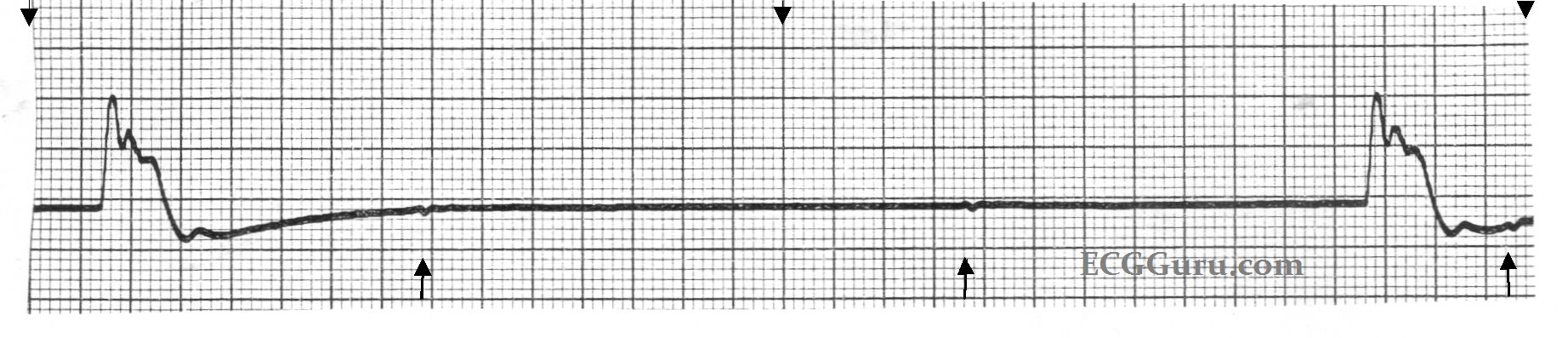
This example of sinus arrest, also called sinus pause, shows a spontaneous return to sinus rhythm. There are many mechanisms by which pauses can occur on the ECG. One concept for beginner students to grasp is that, if the pause contains the equivalent of regular R-to-R intervals, and the first complex after the pause is "on time", we can expect that the sinus node kept firing, but did not penetrate the atria (exit block). If the pause is irregular in length, with the first beat after the pause seeming to come in randomly, we can call this sinus arrest or pause, understanding that there are many different mechanisms that can be at work here. Because what little we can see of the underlying sinus rhythm is irregular, or speeding up, we cannot discern absolutely that this is sinus arrest.
The bottom line for the patient, and for any level practitioner, is, "how is the patient tolerating this pause, and what does it mean to the patient's overall prognosis? In the short term, the patient may require emergency pacing while the cause of the dysfunction is investigated. If pauses are long enough to lower cardiac output, they can cause fainting. More than a few automobile accidents have happened as a result of this type of dysrhythmia.
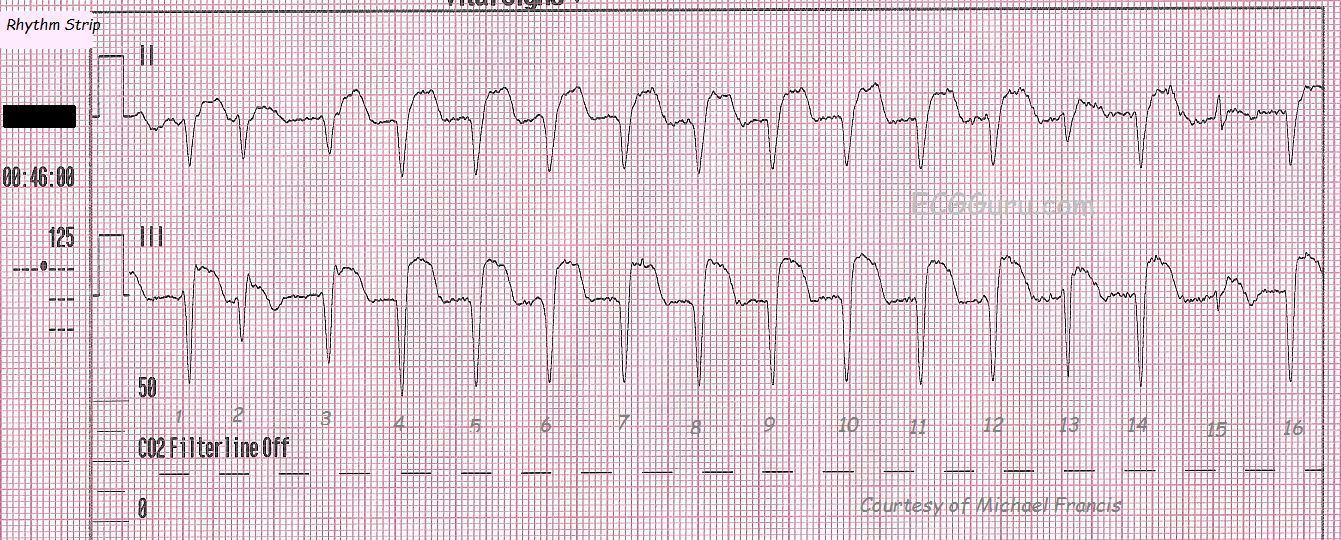
For more advanced students, this short rhythm strip (Lead II) reveals sloping ST depression, and indicates the urgent need for a 12-lead ECG and other tests.