
Submitted by Dawn on Sun, 06/21/2015 - 11:31
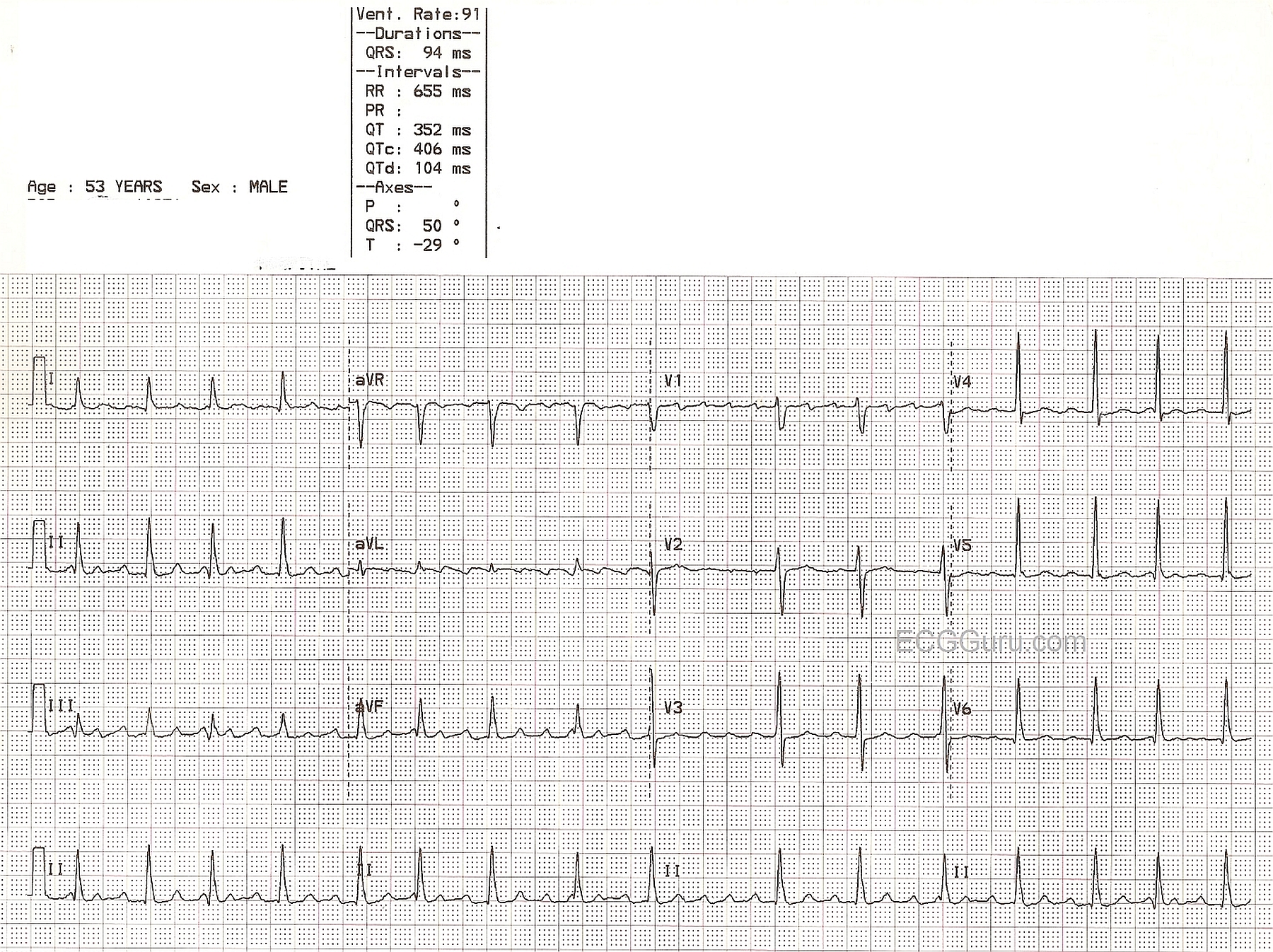
This is a good example of atrial flutter with variable conduction in a 53-year-old man. He had been treated for a fast rate, and now has a rate of approximately 90 per minute. No other clinical information is available. One of the good teaching points in this ECG is that some leads show P waves (or, in this case, flutter waves) better than others. The diagnosis of atrial flutter can be missed by practitioners utilizing only one or two leads.
The typical flutter waves, at a rate close to 300 / min., can best be seen in Leads II, III, aVF, aVL, V1, and V3. Leads II and aVF are especially good for teaching students to "march out" the flutter waves through the entire strip. They can be seen in the QRS complexes and T waves in these leads.
Because atrial flutter often accompanies a diagnosis of congestive heart failure, this is a good ECG for teaching the contribution of rate - atrial and ventricular - in the workload and cardiac output of the patient.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
AFlutter with a Variable Ventricular Response
In Summary — I favor designation of the rhythm seen here as, AFlutter with a controlled but Variable Ventricular Response.
Ken Grauer, MD www.kg-ekgpress.com [email protected]
atrial flutter
Interesting topic and comment, as usual!
Do you suggest to mention the type of atrial flutter (typical vs atipical) when interpreting a given ECG?
Mario Parrinello
Answer to Mario
Hi, Mario,
We apologize that we just now became aware of your question - somehow the notification process on our website broke down.
The answer to your question depends upon your role and your goals. If you are a cardiologist teaching a group of medical students, you would want to mention whether you feel the atrial flutter is typical or atypical. If you are a paramedic reporting the rhythm to the ER physician, it is probably not at all necessary.
Dawn Altman, Admin