
Submitted by Dawn on Sun, 05/05/2013 - 16:26
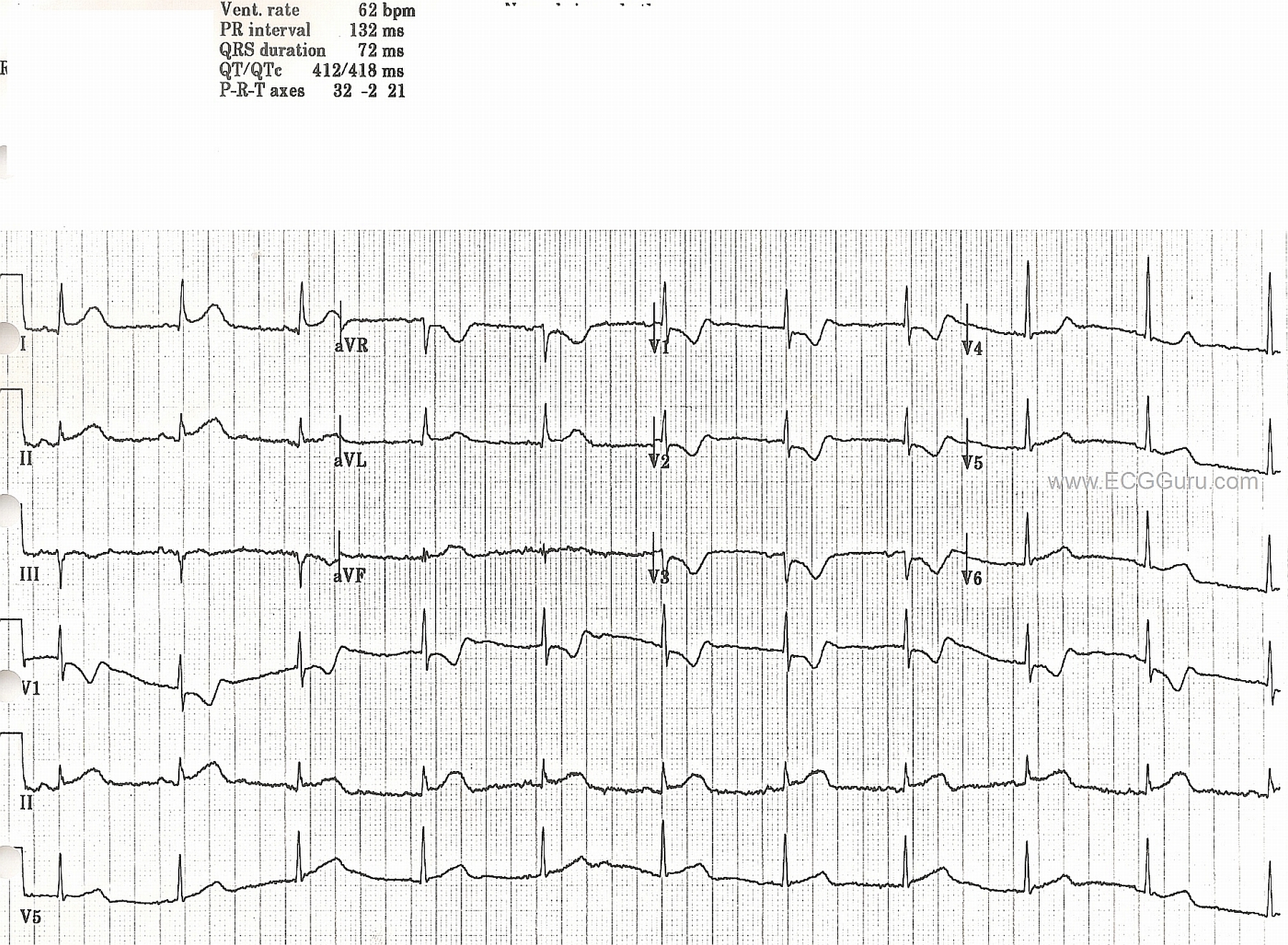
This ECG is from old files, and no patient information is available. Acute ST elevation is apparent in lateral leads I and aVL, and in Lead II. In addition, the anterior leads V1, V2, and V3 show reciprocal ST depression and, in V1 and V2, taller-than-normal R waves. This points to acute posterior - lateral M.I., probably due to occlusion of the circumflex artery. Unfortunately, we do not have angiogram confirmation for this.
The P waves are interesting. They are hard to see because of their small size and the fine baseline artifact present. The best view appears to be in the Lead II rhythm strip at the bottom. In this view, the P waves' morphology appears to be changing. What do you think?
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
SUPERB Example of Acute Postero-Lat MI / Circumflex Occlusion
This tracing is as good as it gets for teaching. Dawn alludes to many of the interesting points. I'll add the following observations:
Ken Grauer, MD www.kg-ekgpress.com [email protected]
Late to the game
I'm late to the game here (reviewing some PWMI cases I have saved) but I just noticed that it looks like V1 and V3 were probably swapped. It accounts for the strange R-wave progression and also the presence of such well-defined p-waves in "V3."
Vince D
http://www.medialapproach.com
Electrode swap
Agreed!
Dawn Altman, Admin