
Submitted by Dr A Röschl on Fri, 01/03/2025 - 03:32
This ECG is from a 65-year-old woman who had previously had no cardiac abnormalities but has now suffered several syncopes within 2 weeks. During the last syncope she suffered a fracture of the left femur.
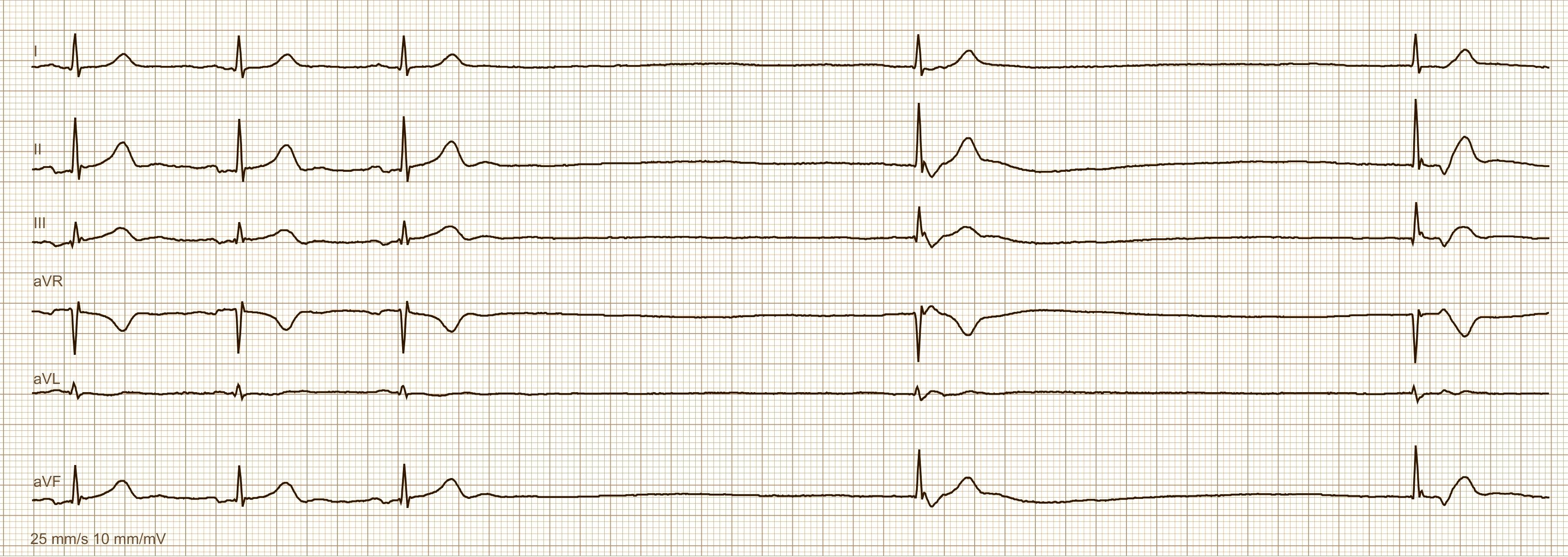
The ECG initially shows a normo-frequent sinus rhythm with an HR of just under 60 bpm. Then the sinus rhythm breaks off (sinus node arrest) and there are 2 pauses of more than 3 seconds, each of which is interrupted by a junctional escape beat. The junctional beat can be recognized as follows: Slightly altered QRS morphology compared to sinus rhythm with the electrical axis remaining the same. The QRS complexes are still narrow. A negative deflection can be seen directly behind the QRS complex, which corresponds to a retrograde P wave. The junctional center can therefore conduct downwards into the ventricles (a QRS complex is formed) and upwards (retrograde atrial excitation = negative P waves in the inferior leads). Such ECG changes are rarely seen in a 12-lead ECG (here 6-lead ECG), more often in a Holter ECG. The clear consequence here is implantation of a permanent pacemaker.
Rate this content:
-

- Dr A Röschl's blog
- Log in or register to post comments
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.