
Submitted by jer5150 on Sat, 11/03/2012 - 18:46
This is a "Routine" resting 12-lead ECG I performed on a patient several months ago in the Outpatient ECG Lab.
PATIENT CLINICAL DATA:
72-year-old white man; asymptomatic; resting comfortably in recumbent position.
This is an exercise in "anomalous" beats.
QUESTION:
(1.) Specifically, what are 3rd, 4th, and 10th beats?
You may wish to review another ECG that I performed I few years ago: http://www.ekgguru.com/content/sr-ectopy-pac-non-cond-pac-pvc-ventricular-escape-laddergram
Rate this content:
-

- jer5150's blog
- Log in or register to post comments
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
3rd beat: PVC
3rd beat: PVC
4th beat: Ventricular escape beat
10th beat: PAC with LBBB aberrancy.
Thank you, Zafer
zafer karabulut
Agreed
I agree with Zafer. The 10th QRS shows a premature ectopic P wave preceding it and partially hidden in the preceding T wave, clinching the interpretation of aberrancy. Although similar in morphology to the first 2 FLB's (funny looking beats), it is not exactly the same. I think the difference is enough to justify saying they come from different sites.
Walter A. Mueller, CCT, CRAT
Agree
I Agree on the 3rd and the 4th beat, and isn't it a retrograde P-wave we see in the T-wave of the 3rd beat?
About the 10th beat, I recall reading somewhere that PAC with aberrancy would show PQ-prolongation, which I cannot see here (using the V1-tracing). I do, however, see a notching in the T-wave of the 9th beat, suggesting PAC, so I may very well be wrong, though..
Cheers
Simon M
INTERPRETATION
INTERPRETATION:(1.) Sinus rhythm (rate about 64/min) with . . .
(2.) . . . LAHB (QRS axis about -49°)
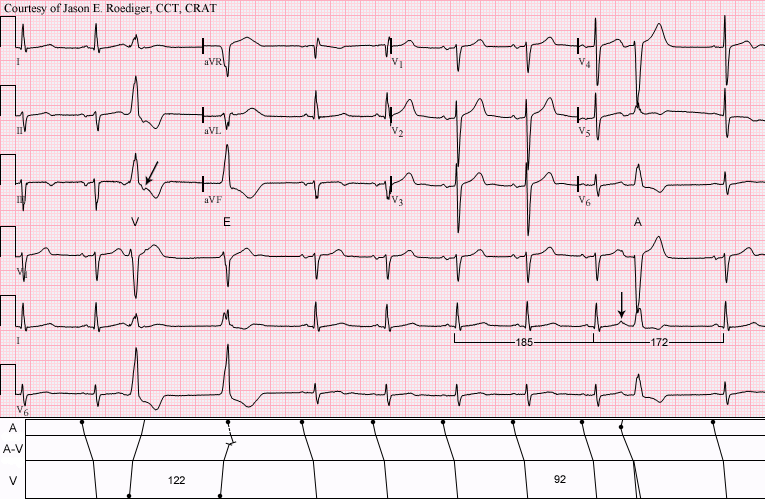
(3.) One VPB (V; 3rd beat) with retrograde atrial activation and presumably originating from the right ventricle (RV).
(4.) One ventricular escape beat (E; 4th beat) also apparently originating from the RV.
(5.) One APB (A; 10th beat) with LBBB aberrancy (see laddergram)
COMMENTS:
When analyzing bundle-branch blocks, the 3 leads with the highest diagnostic yield (in order of importance) are V1, V6, and I. Note, in the bottom 3 monitoring leads, that leads I and V6 are of virtually no help in differentiating QRS morphologies however lead V1 has a wealth of information to help us.
The 3rd beat is a VPB (V) with retrograde ventriculoatrial (V-A) conduction (oblique arrow in lead III). Notice that V-A conduction is comparable to atrioventricular (A-V) conduction with both normal R-P’ and P-R intervals of about 0.17s. On the VPB, the duration of the QRS interval is wider (about 0.14s) than it is on the aberrant APB (0.12s).
Immediately following the VPB, the ensuing post-extrasystolic beat is a ventricular escape (E) and is recognized by the fact that it occurs at the end of a ventricular cycle (122) that is longer than the basic sinus cycle (92). The VPB is considered to be a “forced” beat whereas the ventricular escape is a “passive” beat.
The 10th beat is an APB (A) with LBBB aberrancy. There are several clue to aid our eye:
1. The presence of a preceding P’-wave. Compare the preceding deformed T-wave (vertical arrow in lead I) to all of the other surrounding T-waves with smoothly curved and rounded contours.
2. QRS morphology: See last paragraph below.
3. Less-than compensatory pause: APBs are often followed by a less-than compensatory pause whereas VPBs are usually followed by a fully-compensatory pause. Here the length of the post-extrasystolic cycle is less-than compensatory. It cannot be determined what kind of compensatory pause immediately follows the VPB since the returning beat is a ventricular escape.
The ectopic atrial impulse, of the APB, discharges and resets the S-A node thereby causing overdrive suppression. The P-wave morphology on the last conducted beat is somewhat altered and the possibility of an atrial escape beat should be considered however this is sometimes seen in the returning sinus P-wave of the first post-ectopic beat. Dr. Edward Chung eponymously referred to this as Chung’s phenomenon.
Since the topic was brought up, it should be noted that aberrant APBs can conduct with either normal or prolonged P’-R intervals. If both RBBB and LBBB aberrant APBs are observed in the same patient, usually the LBBB aberrant APBs will demonstrate longer P’-R intervals than the APBs with RBBB aberrancy.
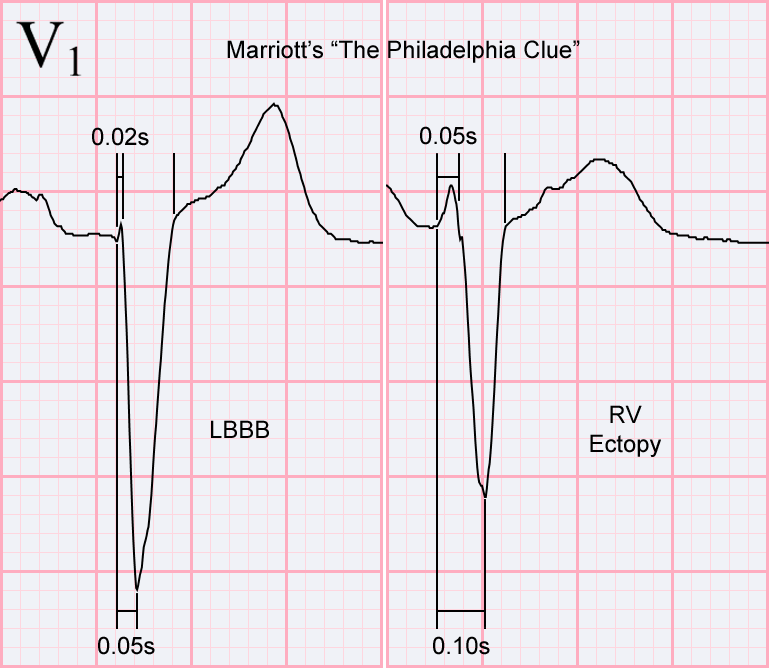
By utilizing Dr. Marriott’s so-called “Philadelphia Clue”, we are able to differentiate between LBBB aberrancy and RV ectopy on predominantly negative QRS complexes in lead V1.
1. Duration of the initial r-wave’s width: The VPB has a wide, little r-wave of 0.05s and the ventricular escape has a wide, little r-wave of 0.06s. Conversely, the APB has a narrow, little r-wave of nearly 0.02s.
2. The presence of a delayed nadir or an early nadir: The VPB has a delayed nadir of 0.10 and the ventricular escape has a delayed nadir of 0.11s. The Life in the Fast Lane website calls this clue the "Brugada sign". Conversely, the APB has an early nadir of 0.05s.
3. The presence or absence of notching and/or slurring: The VPB has some notching/slurring on the downstroke of the S-wave. The Life in the Fast Lane website calls this clue the "Josephson sign". Conversely, the LBBB has a smooth, sleek, and clean downstroke on the S-wave. There appears to be some subtle slurring on the upstroke of the S-wave of the APB.
ACRONYMS / ANNOTATIONS:
APB / A = atrial premature beat
E = ventricular escape beat
LBBB = left bundle-branch block
LAHB = Left anterior hemiblock
RV = right ventricle
VPB / V = ventricular premature beat
Jason E. Roediger - Certified Cardiographic Technician (CCT)
[email protected]