
Submitted by jer5150 on Tue, 07/09/2013 - 12:24
No information available about this patient. What is your interpretation?
Rate this content:
-

- jer5150's blog
- Log in or register to post comments
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
my thoughts...
Sinus rhythm with blocked PACs resulting in assistance from pacemaker.
Just my take
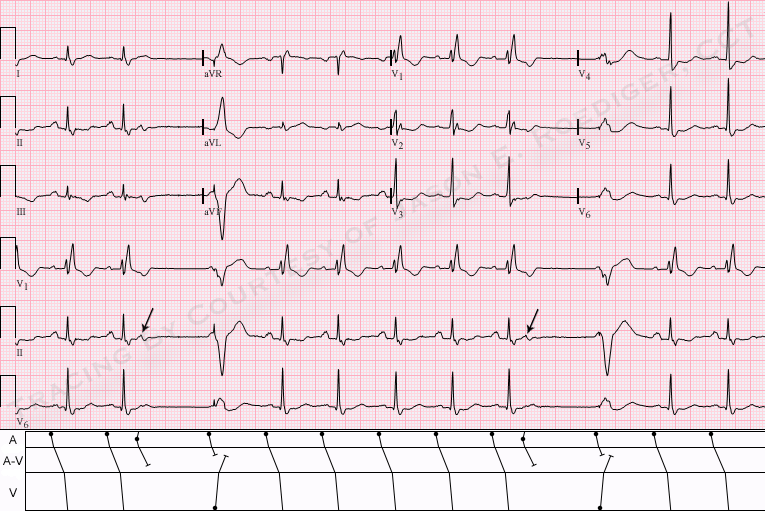
I see a sinus rhythm with a normal axis, with a pause following a ventricular paced beat. V1, V2 have a RBBB morphology with poor r wave progression in the precordial leads.
Blocked PAC - Paced Escape - RBBB with ST Changes
As per my "subject heading" - this NEAT tracing by Jason has a number of interesting findings on it.
NICE tracing! THANKS for posting - : )
Ken Grauer, MD www.kg-ekgpress.com [email protected]
INTERPRETATION
INTERPRETATION:
(1.) Sinus rhythm (rate about 79/min) interrupted twice by . . .
(2.) . . . nonconducted atrial premature beats (APBs; arrows).
(3.) Ventricular demand pacemaker presumably pacing the right ventricle (RV) at a rate of 50/min.
(4.) Right bundle-branch block (RBBB).
(5.) Primary ST-T changes.
COMMENTS:
If not for the nonconducted APBs, we would have no direct way of knowing this patient had any device implanted. As Ken stated, the pacemaker is serving as an artificial analogue for a ventricular escape beat. Playing the part of devil's advocate, my only question would be if a pacemaker was implanted solely because of the nonconducted APBs. Was a pacemaker really necessary? In some patients, it is actually less risky to implant a permanent pacemaker than it is to medically treat the APBs.
Jason E. Roediger - Certified Cardiographic Technician (CCT)
[email protected]