
Submitted by Dawn on Fri, 08/29/2014 - 17:15

This 88-year-old woman was brought to the Emergency Department in cardiogenic shock. Very little is known of her past medical history, but it was relayed to the EMS responders that she had been ill for about four days, when she became much worse.
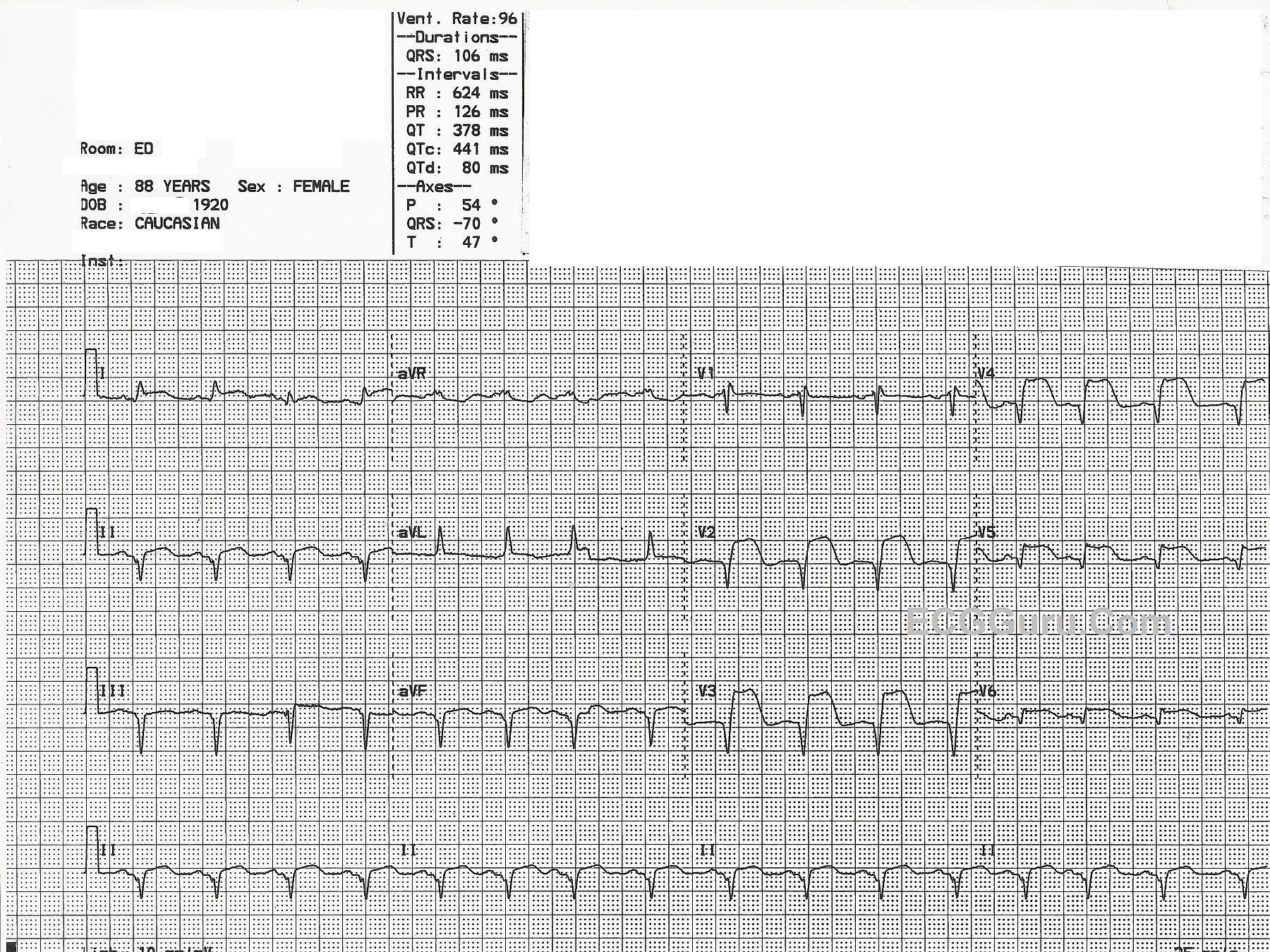
This ECG shows a large, acute anterio-lateral wall M.I., as evidenced by the ST ELEVATIONS in V2 through V6, Leads I and aVL. To make matters worse, there are PATHOLOGICAL Q WAVES in Leads V2 through V6. Pathological Q waves indicate areas of necrosis. Because the myocardium facing the positive electrode is not electrically active, we "see through" the dead tissue to the myocardium on the opposite side of the heart. Pathological Q waves could be thought of as "reciprocal R waves". This represents a great deal of dead myocardium, which will be akinetic - not moving.
To make matters worse, she has pathological Q waves in the INFERIOR WALL as well, in Leads II, III, and aVF. Her ST segments in those leads are flattened and possibly slightly elevated, but not much. There are no reciprocal ST depressions in I and aVL, because they are affected by the anterior - lateral wall M.I., and are elevated.
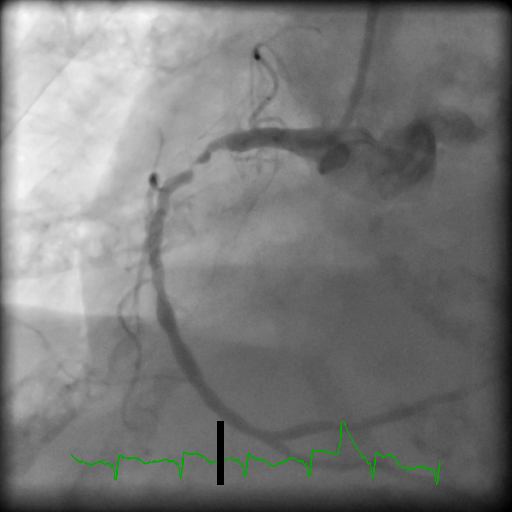
The accompanying photos show her left coronary artery angiogram indicating severe coronary artery disease and a "missing" left anterior descending artery. This is due to a proximal lesion that occurred around the area of the first diagonal artery, cutting off blood flow to a very large part of her anterior-lateral wall. The photo of the right coronary artery shows a very tight lesion which is allowing some blood to pass. The Interventionalist felt that this represented a resolving 100% occlusion (remember, she had been sick for four days). As the blood clot broke up, blood flowed again, lowering the ST segments. Unfortunately, permanent damage had already been done, and she had Q waves in the inferior wall also. This leaves very little of her heart beating, and it is easy to understand why she presented in shock. She suffered cardiac arrests several times during the procedure, and was managed with a balloon pump and ventilator.
Unfortunately, this type of injury is not survivable, and she died in the CVICU a few hours after her procedure. She contributes to our education by demonstrating the cumulative effects of M.I., especially when permanent damage occurs. For a look at her ventriculogram, to understand the devastating effects of these injuries, go to our You Tube channel.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Cardiogenic Shock in an 88yo Woman-ECG, illustrative Cath Films
Ken Grauer, MD www.kg-ekgpress.com [email protected]