
Submitted by jer5150 on Sun, 11/17/2013 - 09:43
Sticking with the same general theme from my last ECG Challenge for the months of September and October, 2013. This is more of a back-to-basics for some readers but will still challenge others. No information for this patient other than it was an adult. How would you interpret this?
Rate this content:
-

- jer5150's blog
- Log in or register to post comments
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Nice case
I think this ECG shows regular sinus P waves at a rate of 50/min, with normal PR interval, narrow QRS, normal QTc, no significant ST-T changes and narrow Q waves in III, aVF, V6 (normal variant). There is incomplete RBBB pattern in V1.
There are two premature ventricular complexes (wide, bizzare, no p wave in front of them if I see correctly). The first one has blocked the P wave after it - the P wave is nonconducted due to concealed conduction.
The second PVC is interpolated (it doesnt disturb the R-R) interval.
Final interpretation: Sinus bradycardia with 2 PVC (2nd one is interpolated). Normal ECG. THANKS for presenting!
Q-wave
But can we still call this a normal-ish ECG in spite of that rather deep Q-wave in III?
Vince D
http://www.medialapproach.com
PVCs
ECG shows
1) Sinus bradycardia with rate around 50 bpm
2) Beat #3 and #7 are PVCs
3) Compensatory pause after the first PVC
4) Second PVC is sandwiched between two sinus beats. Notice that the beat #8 after this PVC manifests a longer PRI than the others.
This is because the PVC travels retrogradely into AV node prolonging the AV node conduction time
Please enlighten
Ryan
PVCs
I agree with sinus rhythm at about 50 bpm... The sinus rhythm is regular throughout. Immediately following the first PVC is a P wave that is not conducted because the ventricles have not yet recovered. Following the second PVC is another P wave on time, but this time it conducts with a longer PR interval. I believe that this PVC comes slightly earlier than the first, and this timing allowed the ventricles to recover with a prolonged PRI.
Thoughts?
Interpretation for last months' ECG Challenge
To see Jason's interpretation of the Sept / October ECG Challenge, follow the link in this month's Challenge.
Dawn Altman, Admin
Hi
Sinus bradycardia
Unifocal vpc
INTERPRETATION
INTERPRETATION:
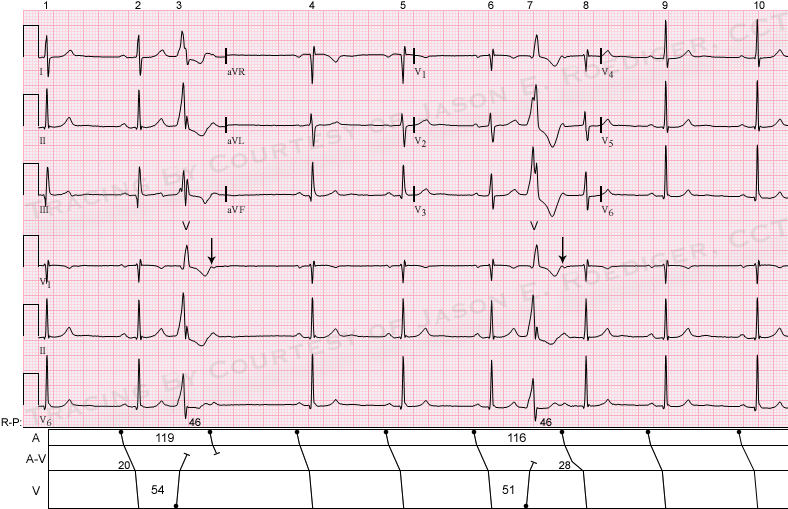
(1.) Slightly irregular sinus bradycardia (48-53/min) with . . .
(2.) . . . two unifocal ventricular premature beats (VPBs); the 1st VPB (3rd beat) being conventional and the 2nd VPB (7th beat) being interpolated with . . .
(3.) . . . retrograde concealed conduction.
COMMENTS:
The first VPB is conventionally followed by a fully-compensatory pause. The Both VPBs (V) are followed by identical RP intervals of about 0.46s. The first VPB has a coupling interval of about 0.54s and the second VPB has a slightly shorter coupling interval of about 0.51s. While its true that neither VPB conducts all the way back up to the atria, I would postulate that the first VPB does conduct further retrogradely into the A-V node leaving it more refractory than the second VPB which probably doesn't conduct as far backwards (see laddergram). Since the second VPB doesn't travel backwards as far, this leaves the A-V node somewhat less refractory so that conduction is possible but still delayed. Compare the P-R interval on the 8th beat to P-R interval (0.28s) on the 2nd beat (0.20s). In other words, the duration of the VPB's preceding coupling interval is directly proportionate to the amount of retrograde concealed conduction it exerts on the A-V junction. The reason the RP intervals are identical despite the non-fixed coupling intervals is because the sinus cycle shortens (119 to 116) by the same amount that the coupling interval shortens (54 to 51) with a difference of 3 for both. Interpolated VPBs are much more likely to be seen in sinus bradycardia than in either sinus rhythm or sinus tachycardia. As far as the deep Q-wave in lead III that Vince mentioned, I'll have to investigate the significance of that and update this post in the near future.
Jason E. Roediger - Certified Cardiographic Technician (CCT)
[email protected]