
Submitted by Dawn on Fri, 10/04/2013 - 23:07
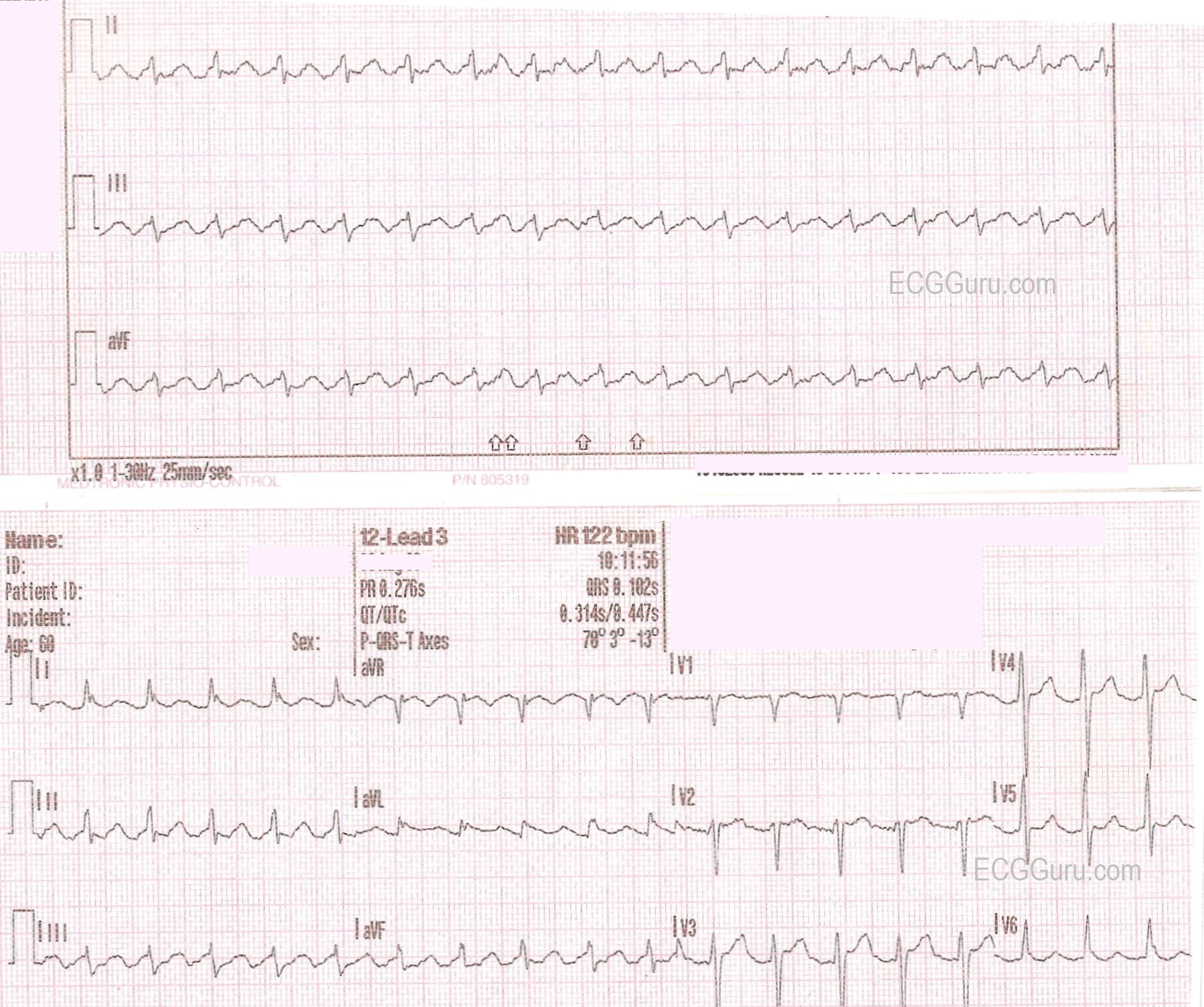
Unfortunately, we have no clinical information on this patient, not even age or gender, as the ECG machine defaults to "Age 60". The rhythm is a supraventricular tachycardia at a rate of about 260/min. with 2:1 conduction, resulting in a heart rate of about 130 / minute. Some would call this atrial tachycardia, and some atrial flutter. Since the reentrant pathways involved in the two rhythms are different, it is probable that an electrophysiologist could determine the exact location of the pathway in the EP lab. Without benefit of this test, we use our best guess. We will leave it to our more advanced Gurus to debate the origins of this rhythm.
The fast P waves are best observed in the limb leads, with one P wave occuring in the QRS complex. If you ignore the QRS complexes for a moment, you can draw an unbroken line through them, uncovering the flutter waves. SVTs with 2:1 conduction can easily be mistaken for sinus tachycardia. Always suspect and look for atrial flutter when the heart rate is around 150 / minute. A 12-lead is a big help, as flutter waves show up better in some leads than in others. Another way to uncover atrial flutter is to slow the rate with vagal maneuvers or medication to decrease the conduction ratio, and observe several flutter waves in a row without QRS complexes.
Of even more concern to this patient may be the ST elevations - slight but noticeable - in Leads V2 - V4, and possibly I and aVL. The J points (the beginning point of the ST segment) can be obscurred by the P wave lying beneath the QRS, and it may be difficult to judge ST elevations.
We expect this ECG to elicit many opinions - possibly different from ours. Please add your comments below. We will enjoy the discussion.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Regular SVT at 130/minute - AFlutter vs ATach
Nice illustrative tracing by Dawn. I agree entirely that best policy is to first describe what is seen rather than venturing diagnoses. As per Dawn - there is a regular SVT at ~ 130/minute. There is atrial activity - but it is clearly not sinus activity since there is no consistent upright P wave in lead II. So best initial description of this rhythm is: "a regular SVT @130/minute without clear sinus activity".
Otherwise - while there may be some ST elevation in anterior precordial leads on this tracing - the ST segment looks to be of upward concavity and less like an acute injury pattern. Overlap with atrial activity probably contributes to the ST segment abnormality. Repeat ECG after termination of the tachycardia should be revealing. I suspect that precordial ST segments will not be of concern.
-----------------------------------------------
Ken Grauer, MD www.kg-ekgpress.com [email protected]
Test Subject from app
Test