
Submitted by Dawn on Sat, 04/27/2013 - 21:38
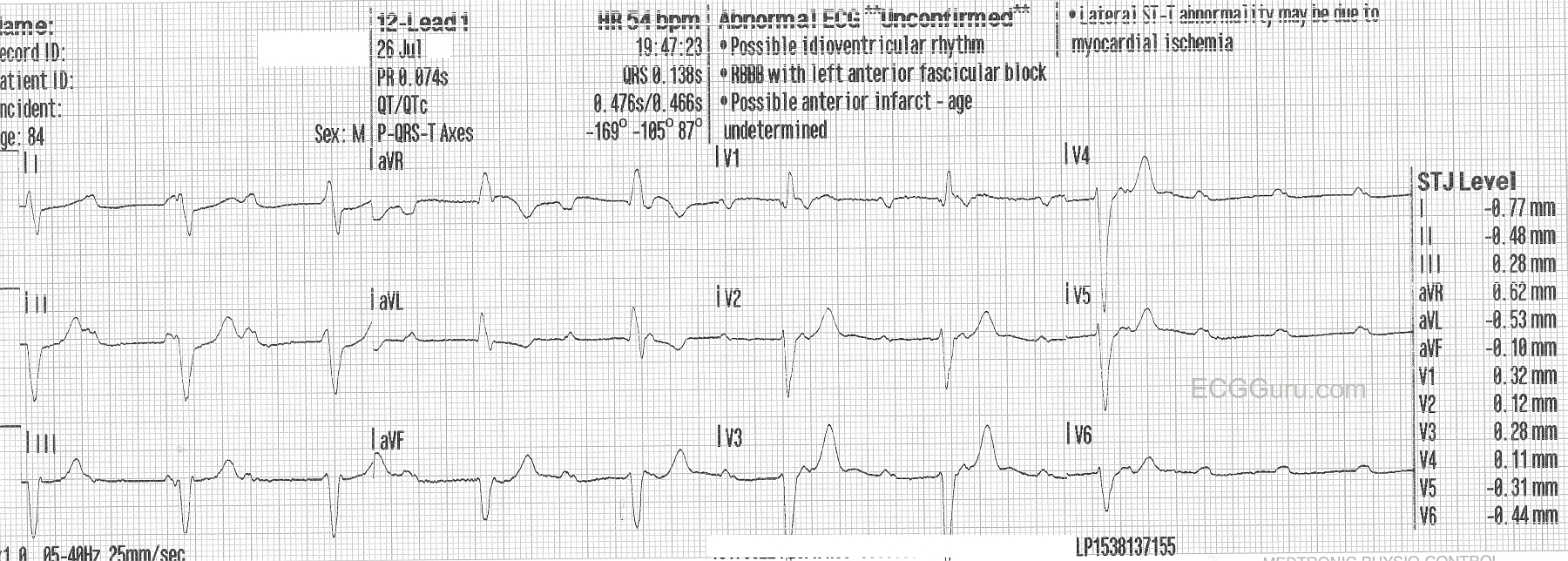
This week's ECG of the WEEK was donated to us by Sebastian Garay. These two ECGs were obtained less than 30 seconds apart from an 84 year-old man who called fire-rescue because he felt dizzy and fell. He was not injured in the fall, and his vital signs remained stable, with an adequate BP. These two ECGs were obtained prior to arrival in the Emergency Dept.
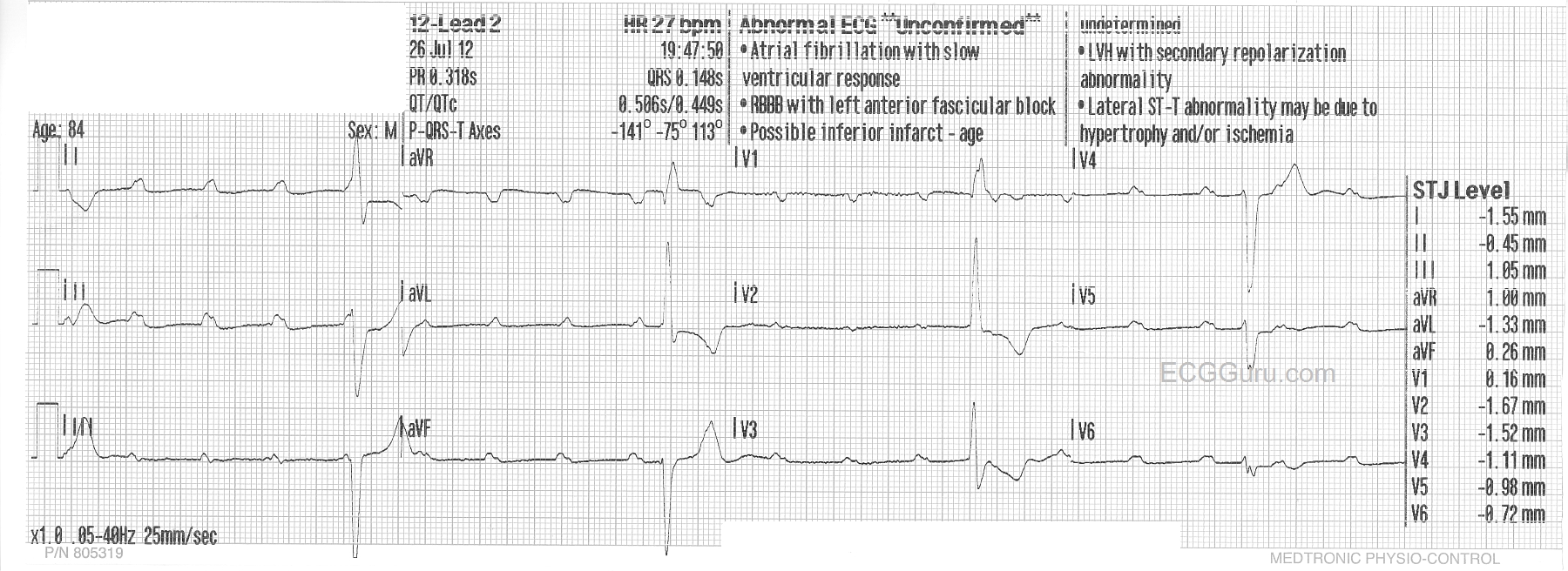
The first one shows a sinus rhythm at about 110/min. There is a complete heart block (third-degree AV block), and the escape rhythm is a wide-complex rhythm at a rate of about 54/min and slowing severely toward the end. The second ECG was taken less than 30 seconds after the first, and shows a significantly slower escape rhythm rate at 27/min., while the sinus rate increases to 120/min. The change is sinus rate is likely an attempt by the nervous system to compensate for the lower cardiac output as the ventricular rate slows. The escape rhythm is not only slower, but there are some changes in the QRS morphology from the first ECG.
For your basic students, this ECG serves to demonstrate the AV dissociation seen in complete heart block. It is easy to "march out" the P waves, and see that some of them are "hiding" in the QRS comlexes. It also shows how quickly a rhythm can change rates.
For your more advanced students, you will want to have a discussion about escape rhythms. This one initially has a fairly fast rate, suggesting junctional origin. The QRS morphology is of the right bundle branch type, with left anterior fascicular block. However, ventricular rhythms originating from the posterior fascicle region can have the "RBBB / LAFB" morphology. If this escape rhythm is fascicular (ventricular) in origin, it is an accelerated idioventricular rhythm. The second escape rhythm appears very similar to the first, with the very noticeable exceptions of QRS morphology, especially in V1 and V2, and the rate.
This patient was given Atropine in the ED, with no change to the rhythm. We do not know what transpired after that, but suspect a pacemaker was in his future.
We look forward to comments from our members about these two very interesting ECGs.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Sequential High-Grade/Complete AV Block Tracings
This is a highly interesting set of tracings (Sebastian's contributions always are! ) - with important teaching/learning points for ALL level providers. I'll make the following observations to add to Dawn's introductory comments:
GREAT set of tracings!
Ken Grauer, MD www.kg-ekgpress.com [email protected]