Our expert today is Darlene Hutton. She has worked in CCU, ICU, PACU, and Emergency as a bedside nurse, educator, and manager. She is currently working as a Clinical Research Manager at Rouge Valley Metabolic Research Associates in Toronto. Darlene also is an Educational Consultant providing workshops, seminars, and conferences on such topics as ECG Interpretation, Dysrhythmia Interpretation, Acute Coronary Syndromes and Cardiology Drugs. She is also an ACLS Course Director and runs courses throughout the province. Her company, QRS Educational Services, founded 18 years ago, provides education to nurses and other health care professionals throughout Canada. She is also the Department Head for Emergency Preparedness in the O.R. in the American College of Plastic Surgical Nursing journal.
Answer:
I PERSONALLY WENT THROUGH THIS 8 YEARS AGO...FUN TIMES. WHEN I WENT TO MY FAMILY DOCTOR HE STATED THE POTENTIAL CAUSES, IN THIS ORDER WERE: ADRENAL TUMOR, CARDIAC DISEASE. THOSE WERE HIS ONLY 2 OPTIONS. NEEDLESS TO SAY, I AM NO LONGER WITH THIS PRACTITIONER. THE 24 HR URINE WAS NEGATIVE AND THE CARDIAC STRESS TEST DID NOT INDUCE THE BIGEMINY, SO THAT WAS ALSO NEGATIVE. IN MY CASE, THE CAUSE CAN BE ATTRIBUTED TO THOSE WONDERFUL HORMONES THAT ACT UP IN THE PERIMENOPAUSAL PERIOD OF OUR LIVES. I TEACH STUDENTS THAT THE HEART DOESN'T NORMALLY THROW OFF BIGEMINY, OR MULTIFOCAL PVCS, OR COUPLETS. WHEN IT DOES, WE MUST ASK OURSELVES "WHY?" COMMON CAUSES ARE: ISCHEMIA (DO AN ECG, THE PATIENT SHOULD HAVE A STRESS TEST AS ANOTHER TEST FOR ISCHEMIA), ELECTROLYTE IMBALANCE (CHECK THE LYTES - HYPERKALEMIA IS ALWAYS A FRONT RUNNER), DRUGS (ONE EXAMPLE IS RED BULL-INDUCED VT IN AN EMERGENCY NURSE WHO DRANKS 3 LARGE CANS DURING HIS 8 HOUR SHIFT).
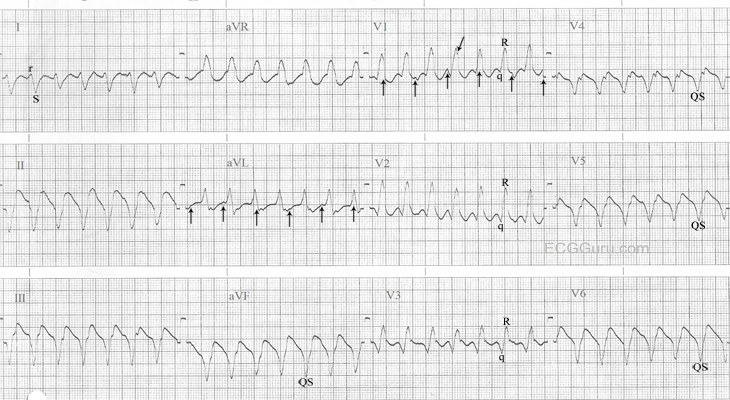
The significance of ventricular bigeminy may be huge or of little consequence. First, it depends on how my patients looks right at this moment. Are they compromized? Some ventricular beats produce an output while others don't. So, when assessing this patient it is important to determine if there is output with these beats; otherwise what may look like a heart rate of 80 may only be one of 40. If all tests have deemed no significant cause of the bigeminy, then there is really nothing more to be done. Starting on an antiarrhythmic drug, such as amiodarone, would not be recommended as this drug may cause worse side effects that the treatment it's being given for; namely torsade des pointe from a prolongation of the QT interval.
Darlene Hutton, RN, BScN, MSN